We hope this information has been valuable to you. If so, please consider a monetary donation to Lifestyle Training Centre via UPI. Your support is greatly appreciated.
Would you like to undergo training for OET, PTE, IELTS, Duolingo, Phonetics, or Spoken English with us? Kindly contact us now!
We hope this information has been valuable to you. If so, please consider a monetary donation to Lifestyle Training Centre via UPI. Your support is greatly appreciated.
Would you like to undergo training for OET, PTE, IELTS, Duolingo, Phonetics, or Spoken English with us? Kindly contact us now!
TEXT A Keratosis follicularis is a genetic disorder that is inherited in an autosomal dominant pattern. Physical examination classically shows keratotic papules that are distributed mostly on the so-called “seborrheic” areas of the body. Nail involvement is not uncommon and is characterized by V-shaped nicking at the distal aspect of the nail bed, longitudinal red and white alternating bands, and subungual hyperkeratosis. Mucosal membrane involvement may occur as white papules on the buccal mucosae, palate, and gingiva with a cobblestone appearance.
Keratosis follicularis affects males and females in equal numbers. It is estimated to occur in 1 in 36,000 to 100,000 individuals in the general population. The disorder usually becomes apparent during the second decade in life, but has developed in individuals as young 4 and older than 70. Keratosis follicularis was first described in the medical literature in 1889.
TEXT B Signs & Symptoms
The symptoms of keratosis follicularis usually become apparent during the teen-age years often around puberty. Symptoms may develop in younger or older individuals, but rarely develop after the third or fourth decade of life. The severity of the disorder and the specific symptoms that develop vary, even among individuals within the same family.
The initial lesions in keratosis follicularis are usually small, firm, greasy bumps (papules) that are often skincolored, brown or yellow-brown in color. The lesions usually affect the areas of the body near sebaceous glands (sebaceous glands secrete oily grease) including the chest, back, forehead and scalp. Darier disease may also affect skin creases e.g. groin.
The skin lesions associated with keratosis follicularis generally develop a brown, greasy crust and become thickened and warty (hyperkeratotic), scaly and darkened. The lesions will slowly grow bigger eventually coming together (coalescing) to form discolored, warty plaques that may cover extensive areas of the body particularly on the trunk. In extremely rare, severe cases, almost the entire body may be affected. The lesions may cause persistent itchiness (pruritus). Some patients have fragile skin that blisters or becomes raw (erosions) and painful.
The skin may develop bacterial, viral or fungal infections (secondary infections) that worsen the condition. Infected skin lesions may give off a distinct, unpleasant (malodorous) smell. The herpes simplex virus may be prone to infecting the lesions and causes pain. Heat, exercise and sunlight may also worsen keratosis follicularis or cause a new outbreak of lesions.
Individuals with keratosis follicularis may have periods when few lesions are present. However, the lesions tend to recur. Keratosis follicularis is usually worse in the summer and improves in the winter. Heat or sun often causes an outbreak.
Another common finding associated with keratosis follicularis is the development of multiple, small, yellow-brown, flattened wart-like (verrucous) bumps (papules) on backs of the hands or feet. These bumps may be the first sign of keratosis follicularis. Many affected individuals develop small horny bumps called punctate keratoses on the palms and soles.
Sometimes the mucous membranes within the mouth develop small bumps (papules). The roof of the mouth (palate) is most often affected. The gums, larynx and esophagus may also be affected. Darier disease can also affect the ducts of the salivary glands causing salivary gland obstruction. In some cases, Darier disease has developed on the mucous membranes of the anus and rectum.
Although in most people Darier disease is limited to the skin, additional symptoms have been reported in some cases including seizures, bipolar disorder, and learning disabilities. Keratosis follicularis may -be restricted to a band of skin on one side of the body (segmental or linear keratosis follicularis).
TEXT C Diagnosis
A diagnosis of keratosis follicularis is made based upon a thorough clinical evaluation, a detailed patient history, identification of characteristic findings and microscopic examination (biopsy) of affected skin tissue. A biopsy may reveal abnormal formation of keratin tissue (keratinization) and failure of cell-to-cell adhesion (acantholysis).
Standard Therapies
Treatment: The treatment of keratosis follicularis is directed toward the specific symptoms that are apparent in each individual. For some individuals, sunscreen, loose clothing, moisturizing creams and avoiding excessive heat may reduce the severity of the disease.
Synthetic derivatives of vitamin A applied directly to the affected areas may help reduce scaly thickening of the skin. Therapy that helps soften and shed hardened, abnormal skin (keratolytics) such as treatment with salicylic acid in propylene glycol gel may also help treat hyperkeratosis. Topical corticosteroids and substances that soothe and soften the skin (emollients) have also been used to alleviate inflammation in localized keratosis follicularis.
Retinoids taken by mouth have been effective in treating individuals with keratosis follicularis and are the drugs most often used to treat severe cases. Oral retinoids such as tretinoin and acitretin affect the entire body (systemic therapy). Oral retinoids can be associated with side effects. Women must not become pregnant when taking a retinoid because these drugs could damage the baby and pregnancy should be avoided for some time after stopping the drug. Retinoids should only be used under the supervision of a physician.
Antibiotics may be necessary to treat individuals with secondary bacterial infection. Antiviral agents such as
acyclovir have been used to treat associated infection with the herpes simplex virus.
Keratosis Follicularis: Questions Questions 1 – 7 For each question 1 – 7, decide which text (A, B, C or D) the information comes from. You may use anyletter more than once.
In which text can you find information about
1. A period of time where keratosis follicularis become evident ___________
2. The share of the disease between genders ___________
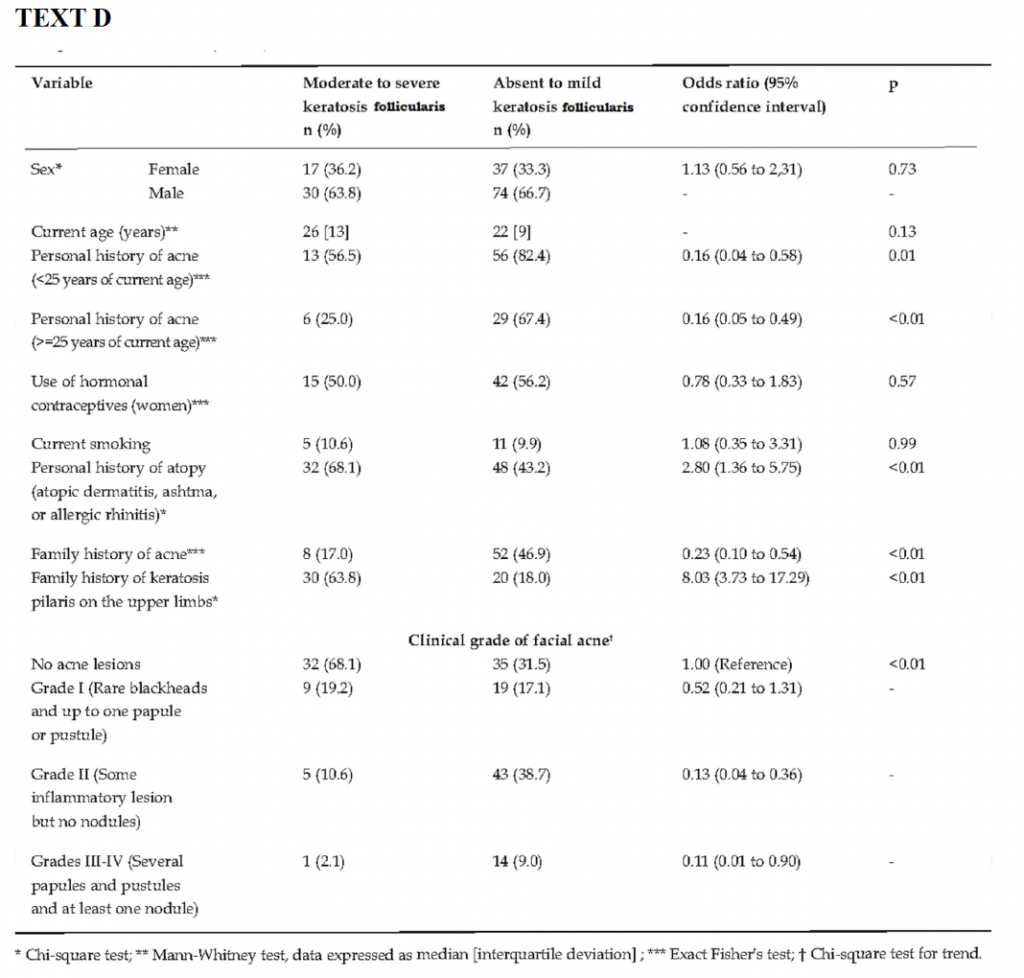
3. A cross-sectional study on keratosis follicularis ___________
4. Ways to reduce the intensity of the disease ___________
5. Infections that can exacerbate the condition ___________
6. Accepted therapy regimen for keratosis follicularis ___________
7. Various grades of acne on the face ___________
Questions 8 – 14
Answer each of the questions, 8 – 14, with a word or short phrase from one of the texts. Each answer may include words, numbers or both.
8. The virus that may be prone to infecting the lesions and causes pain is?
9. What are the causes of keratosis follicularis outbreak?
10. The number of women who used contraceptives who were not diagnosed with keratosis follicularis?
11. What are the small horny bumps called on the palms and soles?
12. Which grade of facial acne had the highest number of people with minimal sufferers of keratosis follicularis?
13. When was keratosis follicularis first described in the medical literature?
14. Which are the drugs taken orally for effective treatment for severe keratosis follicularis?
Questions 15 – 20. Complete each of the sentences, 15 – 20, with a word or short phrase from one of the texts. Each answermay include words, numbers or both.
15. A biopsy may reveal abnormal formation of _________ and failure of cell-to-cell adhesion.
16. _____________ involvement may occur as white papules on the buccal mucosae, palate, and gingiva with a cobblestone appearance.
17. Synthetic derivatives of ____________ applied directly to the affected areas might reduce scaly thickening of the skin.
18. An antiviral agent __________ is being used to treat associated infection with the herpes simplex virus.
19. The percentage of people aged 25 years with the history of acne having acute keratosis follicularis, according to Fisher’s test was ______________.
20. Physical examination shows keratotic papules that are known and distributed mostly on the ____________ areas of the body.
PART B In this part of the test, there are six short extracts relating to the work of health professionals. For questions 1-6 choose the answers (A, B or C) which you think fits best according to the text.
1. The memo is to remind staff. A. to remind them about the statistics of blood flow to the organs. B. the importance of having professional approach during emergency. C. the procedure to give a high quality CPR to patients.
CPR: CPR is a lifesaving intervention and the cornerstone of resuscitation from cardiac arrest. Survival from cardiac arrest depends on early recognition of the event and immediate activation of the emergency response system, but equally critical is the quality of CPR delivered. Both physical and clinical studies demonstrate that the quality of CPR during resuscitation has a significant impact on survival and contributes to the wide variability of survival noted between and within systems of care. CPR is inherently inefficient; it provides only 10% to 30% of normal blood flow to the heart and 30% to 40% of normal blood flow to the brain even when delivered according to guidelines. This inefficiency highlights the need for trained rescuers to deliver the highest-quality CPR possible.
2. The study inform that IE. A. can be reduced by appropriate dental care. B. antibiotics can improve poorer outcomes. C. has revealed no evidences of GI and GU for the cause.
Infective Endocarditis : A study by the members of American College of Cardiology along with other international experts on IE, extensively reviewed published studies in order to determine whether dental, gastrointestinal or genitourinary tract procedures are possible cause of IE. Findings found no conclusive evidence linking GI or GU tract procedures with the development of IE. They also concluded that antibiotics before dental procedures are reasonable only for certain patients at increased risk of developing IE and at highest risk of poor outcomes from IE. The practice of routinely giving antibiotics to patients at risk for IE prior to dental procedures is not recommended except for patients with the highest risk of adverse outcomes resulting from IE. The Committees concluded that only a small number of IE cases might be prevented by antibiotic prophylaxis prior to a dental procedure. In addition, prophylaxis should be reserved only for patients with cardiac conditions associated with the highest risk. You can reduce the risk of IE by maintaining good oral health through regular professional dental care and the use of dental products, such as manual, powered and ultrasonic toothbrushes; dental floss; and other plaque-removal devices.
3. The purpose of these instruction is to explain how A. critical is the patients’ stability. B. to administer pain killers. C. fractures are causes for trauma.
Fracture Diagnosis & Classification Patient Stabilization: Because most fractures result from trauma, it is important to ensure stability of the patient prior to focusing on the fracture. Ideally, for any patient that presents after a traumatic event: 1. Check and stabilize vitals (temperature, pulse quality and heart rate, respiration rate, blood pressure, pulse oximetry), if needed 2. Perform thorough physical, orthopedic, and neurologic examinations. 3. Pursue initial diagnostics, including blood analysis, thoracic and abdominal radiographs, and an AFAST ultrasound. 4. Resolve any life-threatening issues, which means that surgery may need to be delayed for several days due to conditions, such as pulmonary contusions or hypovolemia. 5. Administer proper analgesia as soon as possible: Ideal analgesics are pure mu opioids.
4. Caesarean section is the only way to reduce breech delivery? A. True B. False C. Not Given Vaginal Delivery of Breech Presentation Compared with a foetus with cephalic presentation, a breech foetus faces increased risk during labour and delivery of asphyxia from cord compression and of traumatic injury during delivery of the shoulders and head. Pre-emptive Caesarean section avoids most of this risk. Prior to 1940, despite breech perinatal mortality rates of 5%, CS involved too much maternal risk to be used routinely to lower foetal risk. Improved safety with antibiotics, blood transfusion, and Kerr’s lower segment incision prompted consideration of routine CS for breech presentation. Concurrently, improvements in vaginal breech delivery technique markedly lowered the risk of a trial of labour in experienced hands, and breech perinatal mortality continued to fall, despite stabilization of the CS rate. The debate surrounding the optimal mode of delivery for the breech foetus focuses on a single clinical question: what is the magnitude of risk to the foetus of a TOL and how should we balance it against the increased immediate and future risk of CS to the mother and her future children?
5. What is the main focus of ERIC? A. is to spread the characters Wee & Poo in the schools. B. is to raise cognizance and reduce non healthy habits of children. C. is to calculate the number of students who experience bullying. Tackling Embarrassing Health Problems In the UK an estimated 900,000, or 1 in 12, 5-19 year olds suffer with a continence problem including constipation, soiling, daytime bladder issues and bedwetting. There is also a growing trend of later potty training and children starting school still wearing nappies. At ERIC, we have seen a sharp rise in calls to our helpline regarding children under 6 years old who are struggling with wetting and soiling. Dealing with a toileting problem can have a devastating impact on a child’s learning, development and wellbeing. We must address the reluctance to talk openly about wee and poo. The shame and stigma associated with having an accident can have a long-lasting negative effect on children and teenagers’ school experience. These young people are at high risk of bullying. Education and understanding around the basics of how to keep your bowel and bladder healthy, spotting the signs of a problem and asking for help is vital. These are the issues that need to be normalised and talked about openly to improve children’s physical and mental wellbeing and long-term health outcomes. Based in Bristol, the goal of the schools’ pilot is to raise awareness of good bladder and bowel health for life, using our Wee & Poo characters. It will promote the message that ‘It’s Good to Go!’. In the long term, our ambition is to roll this out as a national campaign targeting all children.
6. The purpose of the study is to explain. A. the recurrence of dislocation can be eradicated with surgery. B. the recurrence rate is between 15% to 44% before treatment. C. the impact it can have on sportsperson after injury.
Primary Patellar Dislocation The average annual incidence of primary patellar dislocation is 5.8 per 100 000 in the general population, with the highest incidence in the 10- to 17-year age group (29 per 100 000). The majority of these patients will not experience further instability, with reported recurrence rates of 15% to 44% after conservative treatment. Although recurrence is the exception and not the rule, many patients continue to be symptomatic following their dislocation episodes. Atkin et al noted that at 6 months postinjury, 58% of patients continue to have limitations with strenuous activity. Failure to return to sport is found in as many as 55% of patients. For these reasons, surgical intervention has been advocated in an attempt to reduce the recurrence rate, which has led to confusion and controversy regarding surgical indications in the acute setting.
PART C Mifepristone at home The World Health Organization’s new guidelines on abortion care recommend that medical abortion in the first 12 weeks of pregnancy can safely be delivered by telemedicine and that women can self-administer both mifepristone and misoprostol at home. Yet on 24 February 2022, the Department of Health for England announced that its temporary approval of home use of mifepristone, made during the covid-19 pandemic, would cease in August 2022. The following day, the Welsh government announced that home use of mifepristone would become permanent, citing the safety and benefits for those accessing abortion services, as well as for the NHS. The Scottish government has yet to decide whether home use of mifepristone will become permanent. Home use of mifepristone was never introduced in Northern Ireland.
Around 80% of all abortions in Scotland, England, and Wales are medical, using mifepristone and misoprostol. Around 80% occur in the first 10 weeks of pregnancy, with the pregnancy ending at home. Scotland introduced legislation permitting women to self-administer misoprostol at home in 2017, followed in 2018 by England and Wales, but legal restrictions meant that women had to take the first dose of mifepristone at a licensed clinical site. This legal requirement was clinically unnecessary and resulted in extra visits for women and extra costs to the NHS.
In recognition of the need to limit transmission of covid-19 from in-person attendances, the governments of England, Wales, and Scotland introduced temporary approvals in March 2020 to allow administration of mifepristone at home. This was the only change made to the law surrounding abortion care and meant that women could collect medication packs to use at home or receive them by post. Evidence based clinical guidance from the Royal College of Obstetricians and Gynaecologists, Faculty of Sexual and Reproductive Healthcare UK, and British Society of Abortion Care Providers emphasises the use of telemedicine and assessment of gestation using last certain menstrual period, with ultrasound conducted only where clinically indicated.
UK guidance has never mandated routine ultrasound scanning to assess gestation or location of pregnancy before abortion, and pre-pandemic guidance from the National Institute of Health and Care Excellence (NICE) already encouraged telemedicine. Registry data for England and Wales show that the new model for delivery of abortion care introduced during the pandemic—a telemedicine consultation, ultrasound only when indicated, and both mifepristone and misoprostol at home—was associated with an increased proportion of abortions being conducted medically and at earlier gestations. This suggests better access to abortion.
Treatment at earlier gestations is less painful and causes less bleeding. Published evidence from England, Wales, and Scotland shows that the new model of care is as safe and effective as former models of in-person consultation and administration of mifepristone on clinical premises. Studies also show that women are able to take mifepristone at home correctly and appreciate the option and privacy of consultation by telephone. Women support continuation of home use of mifepristone for reasons of privacy, convenience, and autonomy. Research among providers suggests they consider the new model more patient centred. An economic evaluation estimates that the telemedicine model saved the NHS at least £3m (€3.6m; $4m) a year.
The English government’s decision to act against substantial clinical evidence, expert advice, and pleas from royal colleges serves only to punish and infantilise women. At a time when reproductive rights in the US and parts of Europe are being attacked, our governments should not be bowing to pressure from anti-abortion extremism. Restrictions to abortion do not prevent abortion; they simply result in later abortion. Telemedicine delivery of abortion care in England will remain, in line with clinical guidelines, and medical abortion at home will continue (as before covid-19), but in England, women will be forced to take one of their pills in clinic rather than at home like their Welsh and Scottish counterparts. This means less flexibility of care in England, less patient centred care, more travel, more time off work for appointments, delays to care, an increase in gestation at abortion, and greater costs to the NHS in England.
Abortion is an essential part of healthcare, and delivery of care should be led by evidence. Governments should act in accordance with the best evidence available for improving public health. This includes following national and international evidence showing that taking mifepristone at home is safe. Sadly, for the English government, home use of mifepristone seems to be the bitterest pill to swallow.
7. What is the disparity about the use of mifepristone in the first paragraph in one of the UK countries? A. Wales government made the use of the medicine permanent. B. It was never instigated in the Northern Ireland. C. Nobody can use the medicine since August 2022 in the UK. D. A non-permanent approval is to be sorted in England. 8. In paragraph 2, which of the following statement is not true. A. England and Wales were preceded by Scotland to legalize the use of medicine without any help. B. 80% of all abortions in the UK countries is done by either of the two medicines. C. National Health Service had to incur extra spendings on the additional visits. D. Scots allowed 10 weeks of pregnant women to get aborted at home in 2017. 9. What is the best practise from the evidence provided from the institutes in England in 3rd paragraph? A. Use telemedicine to assess the menstrual period. B. The medicine mifepristone can be received at home or could be collected. C. A medical examination using a scanner to done if stipulated. D. Scotland was the one to initiate the short-term approval. 10. What point is made by the writer by the use of the word this? A. The neoteric notion. B. Earlier gestation. C. A telephonic data collection. D. Ultrasound before abortion. 11. What do we learn from the study into the new model of care in the 5th paragraph? A. The amount saved by the NHS annually. B. A treatment which has reduced the associated complications. C. Women are indebted due to the secrecy maintained. D. Older type of administration was less effective. 12. What reservation does the write emphasise about restrictions to abortion in the sixth paragraph? A. It will never curb the flaming issue regarding feticide. B. Governments should oblige to the activists. C. Authority should oblige to the recommendations and punish women. D. Abortion is anticipated to be banned in England. 13. What is considered as the stumbling block for women in England post corona period? A. They will be more patient centred than other two countries. B. They will have to visit the health care service for initial services. C. Home based medical abortion will pursue as before covid-19. D. Will incur a huge monetary loss for the patients in England. 14. What does the phrase bitterest pill to swallow refers to in the final paragraph? A. Reliable evidence which is available globally. B. Abortion being and integral part in healthcare. C. The best evidence to improve general health. D. A difficult task faced by the authority in England.
PART C. TEXT 2. Eczema
Eczema, also known as atopic dermatitis, is the most common form of dermatitis. Genetic as well as environmental factors are thought to play a part in the pathogenesis. Eczema is most commonly seen in children but can be seen in adults. People with the disease tend to have dry, itchy skin that is prone to infection. Eczema is commonly known as the “itch that rashes” due to dry skin that leads to a rash as a result of scratching or rubbing. The most important treatment of eczema is skin hydration followed by topical steroids for flare-ups.
People with eczema have a dysfunctional barrier which causes various problems. The cells that make up our skin are essential for optimal skin hydration. People with eczema tend to have dry skin due to the dysfunction in the skin barrier. Water can more easily escape from the skin leading to dehydrated skin. Harmful substances can more readily penetrate the skin due to the dysfunction. People with atopic dermatitis tend to have a skewed inflammatory immune response, and their skin is easily irritated by fragrances and allergens.
The lifetime prevalence of atopic dermatitis is about 15-30% in children and 2-10% in adults. About 60% of cases will develop within the first year of life. The prevalence of atopic dermatitis is more common in rural rather than urban areas. This incidence which emphasizes the link to lifestyle and environment factors in the mechanisms of AD. Atopic dermatitis is apart of the triad known as the ‘Atopic march.’ This relates to the association between patients with atopic dermatitis, asthma, and allergic rhinitis. About 50% of patients with severe atopic dermatitis will develop asthma, and 75% will develop allergic rhinitis.
Research shows there is a genetic component to atopic dermatitis. One common mutation has been observed in the gene Filaggrin, a vital gene for skin cell maturity. This gene is responsible for creating the tough, flat corneocytes that form the outermost protective layer of skin. In a patient with normal skin cells, the corneocytes are tightly packed in an organized manner. A patient with a filaggrin mutation will have a dysfunctional skin barrier due to the haphazard organization of the skin cells. This dysfunction causes a ‘leaky’ skin barrier allowing water loss and decreased protection from harmful substances. People with eczema also have reduced numbers of beta-defensins in the skin. Beta-defensins are host defence peptides that are vital for fighting off certain bacteria, viruses, and fungi. A decrease in these peptides leads to increased colonization and infection, especially with staph aureus.
The histopathology seen in atopic dermatitis is non-specific. In the acute phase lesions, characterized by intensely pruritic, erythematous papules, histopathology reveals mild epidermal hyperplasia, infiltrations of lymphocytes and macrophages along the venous plexus in the dermis and intercellular edema of the epidermis (spongiosis). Lesions biopsied in chronic atopic dermatitis, which are characterized by lichenification and fibrotic papules, may reveal increased hyperplasia and hyperkeratosis of the skin. There is also persistent dermal inflammatory cell infiltrate with lymphocytes and macrophages. The chronic phase lacks the edema or spongiosis that is present in acute phase lesions.
The distribution of the rash seen in atopic dermatitis will vary depending on the age of the person. Infants tend to have widely distributed, dry, scaly and erythematous patches with small excoriations. They also tend to have involvement of their face, especially the cheeks. As the child ages, the rash becomes more localized. Areas affected will include the extensors surfaces such as the wrists, elbows, ankles, and knees. School-aged children tend to follow the pattern that is seen in adults. This pattern includes the involvement of the flexural surfaces usually affecting the anti-cubital and popliteal fosse.
A team-based approach is essential for the care of a patient with atopic dermatitis, especially in moderate to severe cases. Eczema is a common condition seen in pediatric and family medicine offices. Typically patients with mild to moderate eczema can be treated in the office by their primary care provider with standard therapy. Patients with moderate to severe cases may require referral to dermatology for systemic treatments. If a patient is not responding to typical treatment regimens, they may benefit from a consult with an allergist for a patch or skin scratch testing. An interprofessional team of a specialty trained dermatology nurse and specialty-trained dermatology clinician will provide the best patient care.
15. In the first paragraph, the writer says that the issue with people having eczema? A. is commonly known as rashes that can itch. B. are caused by two vital factors. C. severe worsening of the disease. D. are with a tendency to get other conditions. 16. What does the writer mean by the word skewed? A. Distorted. B. Straightened. C. Inclined. D. Assorted. 17. What does the word triad refer to in the third paragraph? A. causes of atopic march. B. link between lifestyle and environment. C. link between the three conditions. D. susceptible areas. 18. In the fourth paragraph, we learn that Beta- defensins are? A. are compounds that decreases colonization and invasion of germs. B. are compounds that fight against the invasion and growth of microorganisms. C. are compounds that decreases protection from harmful substances. D. are compounds that prevent peptides from pathogens. 19. Why does the writer say that filaggrin mutation can be problematic because of? A. the important gene for skin cell maturity. B. the cells of the skin being of unsystematic pattern. C. the research found the genetic component to atopic dermatitis. D. the gene creating a layer as a defence mechanism on the skin. 20. The distinguishing features of chronic phase atopic dermatitis are? A. persistent edema, itchy skin and interconnected blood vessels. B. abnormal redness of the skin and less severe epidermal hyperplasia. C. the study of changes in tissues caused by disease. D. enlarged organs, thickened and leathery skin. 21. What is highlighted regarding the distribution pattern seen in matured population? A. Generally affects the inner flexible space in the knee joint and forearm. B. Most commonly seen on the cheeks. C. Predominantly affects the fronts part of the knee. D. Distribution of rashes are largely of the same proportion. 22. What does the writer states regarding the treatment options for eczema patients? A. Most patients should be treated only by the primary care provider. B. A dermatologist should be consulted for standard treatments. C. A collaborative team effort would be of ultimate benefit for non-responders. D. A co-operative attitude amongst the specialist is beneficial for all patients.
We hope this information has been valuable to you. If so, please consider a monetary donation to Lifestyle Training Centre via UPI. Your support is greatly appreciated.
Would you like to undergo training for OET, PTE, IELTS, Duolingo, Phonetics, or Spoken English with us? Kindly contact us now!