IELTS task 1 Map: City
Sample answer by Lifestyle Training Centre The given map delineates the geographical, population, and infrastructural disparities in a locale between […]
Sample answer by Lifestyle Training Centre The given map delineates the geographical, population, and infrastructural disparities in a locale between […]
Sample answer by Lifestyle Training Centre The provided sketch meticulously illustrates the historical setting from 1980 and the present state
Sample answer by Lifestyle Training Centre The presented diagram delineates the current infrastructure alongside proposed modifications for a specific locale.
In IELTS Writing Task 1, maps are visual prompts that depict the layout or design of a location, such as
In IELTS Writing Task 1, a combination of a bar chart and a table refers to a visual prompt that
In IELTS Writing Task 1, a table is a structured set of data presented in rows and columns, providing information
In IELTS Writing Task 1, a line graph is a type of visual representation that displays data points connected by
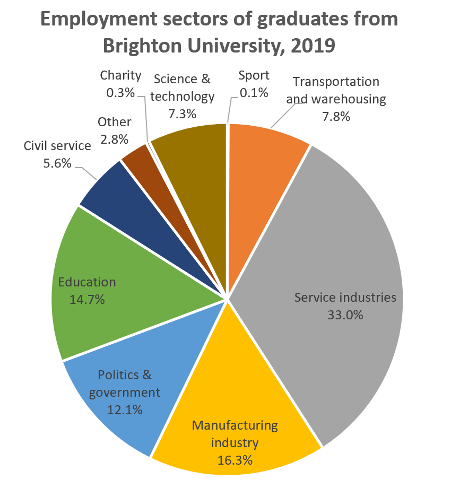
🧾 IELTS Writing Task 1: Pie Chart – Step-by-Step Structure 1. Introduction (Paraphrase the question) 🖋 Example: The provided pie
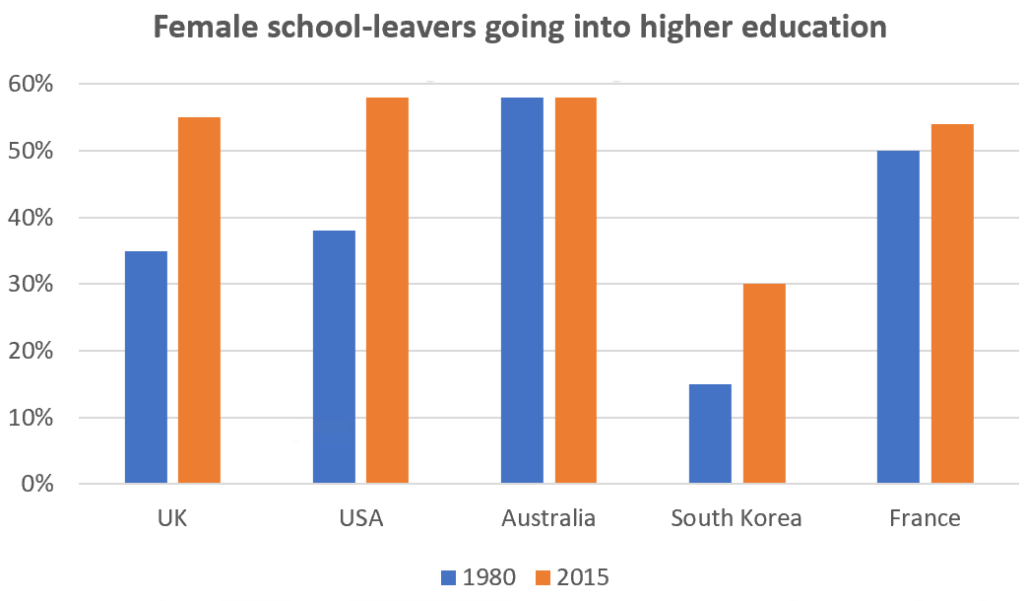
In IELTS Writing Task 1, a bar chart is a graphical representation of data using rectangular bars or columns. Each
Topic: Globalisation. Task 2: Movie Task 3: MoviesCandidate: Subhash (LTC student) This is a live transcript from one of the