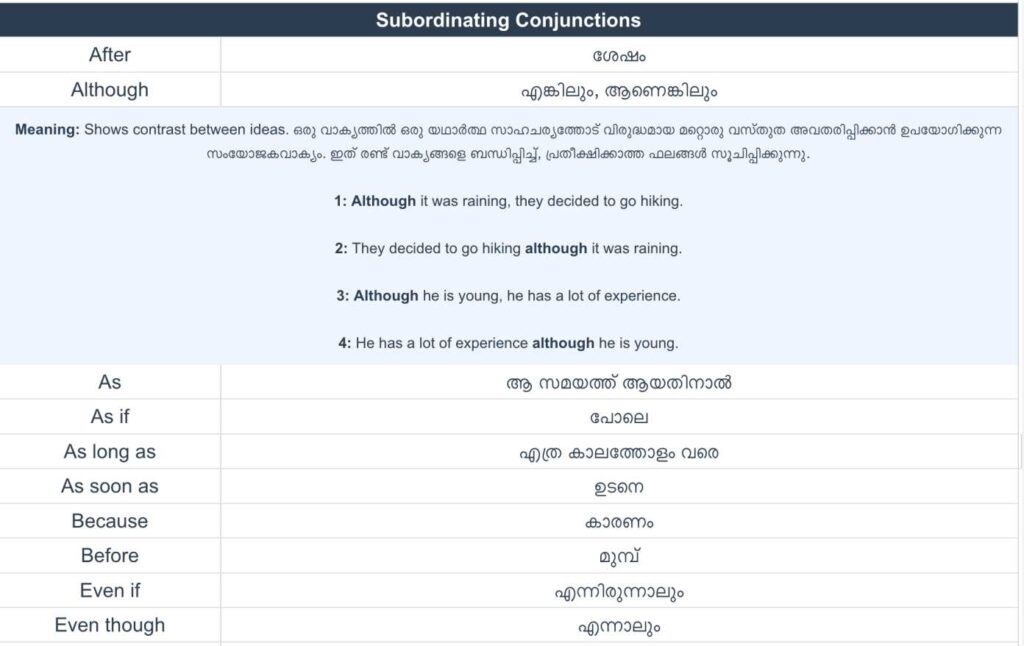
Subordinating conjunctions
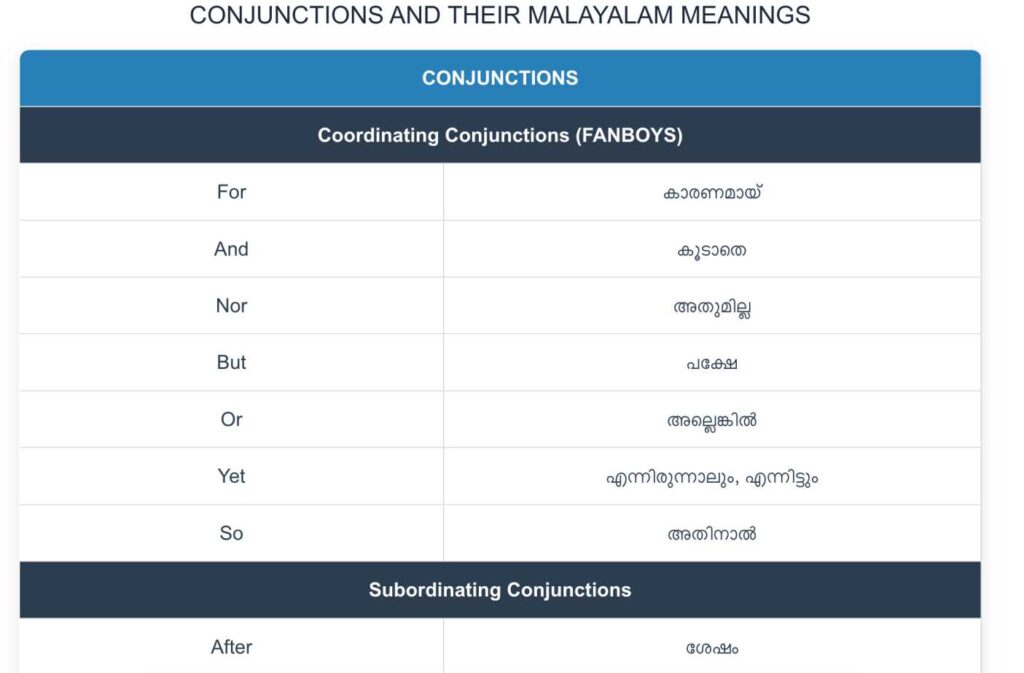
Subordinating Conjunctions (അധീന ബന്ധനങ്ങൾ) Conjunctions – Learn Coordinating, Correlative, Subordinating Conjunctions & Conjunctive Adverbs Conjunctions and Their Malayalam Meanings Conjunctions […]
Subordinating Conjunctions (അധീന ബന്ധനങ്ങൾ) Conjunctions – Learn Coordinating, Correlative, Subordinating Conjunctions & Conjunctive Adverbs Conjunctions and Their Malayalam Meanings Conjunctions […]
Do not start a sentence with coordinating conjunctions. Use them in between Conjunctions – Learn Coordinating, Correlative, Subordinating Conjunctions &
Attempt the test View answers Would you like to download a copy of the practice test? Please click on the
1 38 Green road2 sw183hy3 01289 8473324 2020BD5 21 06 1997 6 d7 f8 a9 2510 next week11 route book12
Attempt the test View answers Would you like to download a copy of the practice test? Please click on the

Answer keys: 1. 0263799785 1 Avalon Drive 2 Jasper Avenue 3 Wednesday 4 (next) Saturday 6. 2 7. A 1 C
Section 1 1.D 2.B 3.C 4.C 5.35C Campus lane 6.garcianuk@email.uk 7.200-250/ 200 to 250 8.D 9.A 10.B Section 2 11.C
ATTEMPT THE TEST ANSWER KEYS Would you like to download a copy of the practice test? Please click on the
1. The Past Five Months2. Basketball3. Non-steroidal Anti-inflammatory4. Arthritis5. Swelling And Tenderness 6. Radial Pulses7. Decreased Flexion8. Decreased Adduction Rotation9.