Do you need printed IELTS/ OET practice material? Place your order today. Available now for just Rs: 1,100 (including shipping all across India) Contact us at our WhatsApp number: +91 9886926773 to place your order. (Free for LTC students)
We hope this information has been valuable to you. If so, please consider a monetary donation to Lifestyle Training Centre via UPI. Your support is greatly appreciated.
Would you like to undergo training for OET, PTE, IELTS, Duolingo, Phonetics, or Spoken English with us? Kindly contact us now!
We hope this information has been valuable to you. If so, please consider a monetary donation to Lifestyle Training Centre via UPI. Your support is greatly appreciated.
Would you like to undergo training for OET, PTE, IELTS, Duolingo, Phonetics, or Spoken English with us? Kindly contact us now!
Do you need printed IELTS/ OET practice material? Place your order today. Available now for just Rs: 1,100 (including shipping all across India) Contact us at our WhatsApp number: +91 9886926773 to place your order. (Free for LTC students)
We hope this information has been valuable to you. If so, please consider a monetary donation to Lifestyle Training Centre via UPI. Your support is greatly appreciated.
Would you like to undergo training for OET, PTE, IELTS, Duolingo, Phonetics, or Spoken English with us? Kindly contact us now!
We hope this information has been valuable to you. If so, please consider a monetary donation to Lifestyle Training Centre via UPI. Your support is greatly appreciated.
Would you like to undergo training for OET, PTE, IELTS, Duolingo, Phonetics, or Spoken English with us? Kindly contact us now!
READING PASSAGE 1. You should spend about 20 minutes on Questions 1-13> which are based on Reading Passage 1 below.
Odonata is the order of insects that includes dragonflies and damselflies. To the human eye, their shining colors1 and delicate-looking wings make them beautiful creatures to behold. In the natural world, however, they are fearsome predators. Dragonflies and damselflies get their name from the powerful serrated jaws they use to tear apart their prey. The word odonata means “toothed jaw.”
Dragonflies and damselflies are often confused with each other because they are very similar. Close observation reveals the differences between them. The most obvious difference is the way they hold their wings while at rest. Dragonflies hold their wings out to the side while damselflies fold their wings back. Dragonflies have very large eyes that seem to cover the entire face because they are so close together that they touch each other. Damselflies’ eyes are smaller, and there is a space between them. Dragonflies are larger and stronger animals than damselflies and fly longer distances. Thus, they can be found in woods and fields away from the water. Damselflies are not such strong fliers and are most often seen around the edges of ponds and streams since they do not normally fly far from the water.
The largest odonata living today are the Hawaiian endemic dragonfly and the Central American damselfly, each of these species having a wingspan of 19 centimeters. The smallest is the libellulid dragonfly, native to east Asia, with a wingspan of just 20 millimeters. Fossils have been discovered that prove that dragonflies have been in existence for over 300 million years. The largest dragonfly fossil ever found belongs to the now-extinct meganeura monyi, which lived 300 million years ago and had a wingspan of 75 centimeters. This giant was a fearsome predator indeed, which feasted on small amphibians as well as on other insects.
Dragonflies and damselflies both lay their eggs on or just below the surface of the water in a pond or stream. Some species lay their eggs on the stem of an aquatic plant. The babies emerge from the eggs in the form of nymphs. They live underwater, breathing through gills and preying upon water insects, tadpoles, small fish, and even other nymphs. They hunt by hiding in the shadows at the bottom of a pond or stream, waiting for prey animals to swim by. They have a special lip that they can extend far forward in order to grab their prey when it comes close. Depending on the species, they live this way for several months or even several years. As the nymph grows, it sheds its skin several times. Finally, it leaves the water and sheds its skin one last time. The adult emerges, ready to live the next few weeks or months on land and in the air. The adults do not live for more than four months, and many species live as adults for only a few weeks.
The exceptional visual abilities and flying skills of dragonflies and damselflies make them very adept hunters. Their special eyes give them a nearly 360-degree field of vision, and they can detect even the smallest movement or flash of light caused by other flying insects. They have two sets of wings that can move independently of each other. This gives them great maneuverability1 in the air, which is important to these creatures because they catch their prey while flying. They can hover, make sharp turns, and fly backward. Some species of dragonflies can fly 60 kilometers an hour or more. Their prey consists of flying insects such as mosquitoes, deerflies, smaller dragonflies, and butterflies and moths. One species of dragonfly takes spiders out of their webs.
Bloodthirsty predators that they are, dragonflies and damselflies are prey for other animals in their turn. The nymphs are eaten by fish, frogs, toads, and other aquatic creatures. In the adult stage, they are hunted by birds, frogs, and larger dragonflies and damselflies. They might also be caught in a spider’s web. What goes around comes around.
Questions 1 -6. Which o f the facts below & we true of dragonflies, and which are true o f damselflies. according to the information in the passage? On lines 1—6 on your answer sheet, write:
A if it is a fact about dragonflies only B if it is a fact about damselflies only C if it is a fact about both dragonflies and damselflies
1 They have sawlike jaws. 2 They hold their wings on their backs while resting. 3 Their eyes have a gap between them. 4 They can be seen in fields at a distance from ponds and streams. 5 The largest species has a wingspan of 19 centimeters. 6 The largest fossil has a wingspan of 75 centimeters.
Questions 7—13. Complete the notes about the life cycle of odonata below. Choose your answers from the box below and write the correct letters, A —K, on lines 7—13 on your answer
The eggs are laid 7________________. The young dragonflies and damselflies, called 8________________ , live underwater for a few 9 ________________. They eat small water animals, catching their food 10 _____________________When they are almost fully grown, they leave the water. The adults live for only a few 11 _________________. They are skillful1 12 _________________ and catch their prey 1 3 ________________
A in the air B with their lips C tadpoles D fliers E near the water’s surface F nymphs G at the bottom of a pond H months or years I weeks or months J swimmers K with their wings
READING PASSAGE 2 You should spend about 20 minutes on Questions 14—26
History of Fire Fighting and Prevention More than two thousand years ago, Roman emperor Augustus organized2 a group of watchmen whose job was mainly to look out for fires and sound an alarm in the event of one. For many centuries that followed, fire equipment was limited to buckets of water that got passed from person to person. The axe was later found to be a useful tool both for removing fuel in large fires and for opening holes to allow smoke and flames to escape from burning buildings. Watchmen also learned to create firebreaks with long hooked poles and ropes in order to pull down structures that provided fuel for a fire. In 1066, in order to reduce the risk of fire in thatched-roof houses, King William the Conqueror made a ruling: Citizens had to extinguish their cooking fires at night. His term couvrefeu, meaning “cover fire,” is the origin of the modern day term curfew, which no longer carries a literal translation.
The event that had the largest influence in the history of fire fighting was the Great Fire of London in 1666. The devastating blaze originated at the King’s Bakery near the London Bridge. At the onset, Lord Mayor Bludworth showed little concern for the fire, assuming it would extinguish itself before he could organize a group of men to attend to it. However, the summer of 1666 had been uncharacteristically hot and dry, and the wooden houses nearby caught fire quickly. Within a short time* the wind had carried the fire across the city, burning down over 300 houses in its path. Although the procedure of pulling down buildings to prevent a fire from spreading was standard in Britain, the mayor grew concerned over the cost it would involve to rebuild the city and ordered that the surrounding structures be left intact. By the time the king ordered the destruction of buildings in the fire’s path, the fire was too large to control. It was not until the Duke of York ordered the Paper House to be destroyed in order to create a crucial firebreak that the London fire finally began to lose its fuel.
When it became clear that four-fifths of the city had been destroyed by the fire, drastic measures were taken in London to create a system of organized fire prevention. At the hands of architects such as Christopher Wren, most of London was rebuilt using stone and brick, materials that were far less flammable than wood and straw. Because of the long history of fires in London, those who could afford to build new homes and businesses began to seek insurance for their properties. As insurance became a profitable business, companies soon realized1 the monetary benefits of hiring men to extinguish fires. In the early years of insurance companies, all insured properties were marked with an insurance company’s name or logo. If a fire broke out and a building did not contain the insurance mark, the fire brigades were called away and the building was left to burn.
The British insurance companies were largely responsible for employing people to develop new technology for extinguishing fires. The first fire engines were simple tubs on wheels that were pulled to the location of the fire, with water being supplied by a bucket brigade. Eventually, a hand pump was designed to push the water out of the tub into a hose with a nozzle. The pump allowed for a steady stream of water to shoot through a hose directly at the fire source. Before long, companies began to utilize water pipes made from hollowed tree trunks that were built under the roadway. By digging down into the road, firemen could insert a hole into the tree-trunk pipe and access the water to feed into the pump.
Fire fighting became a competitive business, as companies fought to be the first to arrive at a scene to access the water pipes. After a series of fires destroyed parts of London, fire-fighting companies were forced to reconsider their intentions. By the eighteenth century, fire brigades began to join forces, and in 1833 the Sun Insurance Company along with ten other London companies created the London Fire Engine Establishment. In 1865, the government became involved, bringing standards to both fire prevention and firefighting and establishing London’s Metropolitan Fire Brigade. Though the firemen were well paid, they were constantly on duty and thus obliged to call their fire station home for both themselves and their families.
New technology for fighting fires continued to develop in both Europe and the New World. Leather hoses with couplings that joined the lengths together were hand-sewn in the Netherlands and used until the latel800s, when rubber hoses became available. The technology for steam engine fire trucks was available in Britain and America in 1829, but most brigades were hesitant to use them until the 1850s. It was the public that eventually forced the brigades into putting the more efficient equipment to use. In the early 1900s, when the internal-combustion engine was developed, the trucks became motorized. 1 This was a timely advancement in fire-fighting history, as World War I put added pressure on brigades throughout the world.
Questions 14-20. Complete the chart below. Use NO MORE THAN THREE WORDS from the text for each answer. Write your answers on lines 14-20 on your answer sheet.
Cause
Effect
Men used poles and ropes to pull down buildings near a fire. Thatched-roof houses burn down easily. At the time of the Great Fire of London, the weather was 16_____________ The Mayor of London thought it would be too expensive to 17_____________ The Great Fire destroyed most of London. There had been many 19_____________in London over time. Insurance companies did not want to pay for rebuilding clients’ houses destroyed by fire.
The fire did not have 14_____________ The King ordered people to 15_____________their fires nightly. The fire spread quickly. He told people not to pull down buildings in the fire’s path. People built new buildings out of 18_____________ People started to buy insurance to protect their homes. Insurance companies hired men to 20_________
Questions 21-23. Choose the correct letters, A—C, and write them on lines 21—23 on your answer sheet. 21 The first fire engines A carried water to the site of the fire. B used hand pumps. C had very long hoses.
22 In 1865, A London was destroyed by a series of fires. B fire brigades began to join forces. C the Metropolitan Fire Brigade was established.
23 Firemen who worked for the Metropolitan Fire Brigade A earned low salaries. B lived at the fire station. C were not allowed to marry.
Questions 24 -26. Do the following statements agree with the information in the reading passage? On lines 24—2 6 on your answer sheet, write:
YES if the statement agrees with the information NO if the statement contradicts the information NOT GIVEN if there is no information on this in the passage
24 Leather hoses for firefighting were made by machine. 25 Steam engine fire trucks were used until the early 1900s. 26 Fires caused a great deal of damage in London during World War I.
READING PASSAGE 3. You should spend about 20 minutes on Questions 27—40> which are based on Reading Passage 3 below.
The Luddites The term Luddite is used to refer to a person who is opposed to new technology. The word derives from the name Ned Ludd, a man who may or may not have actually existed. The original Luddites were textile workers in early nineteenth century England who protested changes brought on by the industrial revolution. These weavers made lace and stockings by hand, carrying out their craft independently in their homes according to traditional methods. In the 1800s, automated power looms and stocking frames were introduced, radically changing the traditional work system. Weavers’ work was moved from individual homes to factories; individuals could not afford to buy the new machines for themselves. The new machines were not difficult to run. They could be operated by unskilled workers and turned out an inferior product, but they produced large quantities cheaply, which was the aim of the new factory owners. The makers of finely crafted, handmade textiles could not compete with the new machines. Instead of continuing their tradition as skilled, independent workers, they would have to go to work in factories for low wages.
The industrial revolution was happening everywhere. In the textile-producing towns of England, workers focused on the new weaving machines as the source of their troubles. The height of Luddite activity occurred in the years 1811-1812. Groups of men, often in disguise, would arrive at a factory and make demands for higher wages and better working conditions. If these demands were not met, the group retaliated by smashing the factory machines. These groups often claimed that they were working under the command of General Ned Ludd, and thus came to be called Luddites.
Who was Ned Ludd? Rumors1 about this mysterious person abounded. He came to be associated with that traditional champion of the poor, Robin Hood. The original Luddite activity was centered2 around Nottingham, and many said that Ned Ludd hid out in nearby Sherwood Forest, just as the legendary Robin Hood had. According to another tradition, Ned Ludd was a weaver who had acci dentally broken two stocking frames, and from that, came to be the one blamed any time an expensive piece of weaving equipment was damaged. Whoever Ned Ludd may or may not have been, riots protesting the new factories were carried out in his name throughout England’s textile-producing region.
Workers’ families suffered as wages fell and food prices rose. There were food riots in several towns, and Luddite activity spread. In the winter of 1812, the Frame-Breaking Act was passed, making the destruction of factory equipment a crime punishable by death. The government sent thousands of troops into areas affected by the riots. In the spring of that year, several factory owners were killed during Luddite riots, and a number of textile workers died as well. Following one of the largest incidents, when rioters set fire to a mill in Westhoughton, four rioters, including a young boy, were executed. In another incident that spring, a group of over a thousand workers attacked a mill in Lancashire with sticks and rocks. When they were beaten back by armed guards protecting the mill, they moved to the mill owner’s house and burned it down. The wave of violence resulted in a crack down by the government. Suspected Luddites were arrested and imprisoned, and many of them were hanged.
By the summer of 1812, Luddite activity had begun to die down, although there continued to be sporadic incidents over the next several years. In 1816, a bad harvest and economic downturn led to a small revival of rioting. In June of that year, workers attacked two mills, smashing equipment and causing thou sands of dollars worth of damage. Government troops were brought in to stop the violence. In the end, six of the rioters were executed for their participation. However, rioting never again reached the levels it had in 1811 and 1812.
The Luddites were short-lived, but they left an impressive mark. They were responsible for destroying close to one thousand weaving machines during the height of their activity in 1811-1812, as well as burning down several factories. Beyond the physical damage, however, they left their mark in people’s minds. The famed English novelist Charlotte Bronte set her novel Shirley in Yorkshire at the time of the riots. This novel is still widely read today. In our present time of rapid technological change, people who are concerned about the pace of techno logical advance often call themselves Neo-Luddites. Although the responses to it may differ, concern about the changes brought on by technology continues.
Questions 27 -32 Match each cause in List A with its effect in List B. Write the correct letter, A—H\ on lines 27—32 on your answer sheet. There are more effects in List B than you will need, so you will not use them all.
List A Causes 27 The new weaving machines were expensive to buy. 28 The new weaving machines were easy to operate. 29 Workers’ demands for better pay and conditions were not met. 30 Rioting spread to many towns. 31 A law was passed against destroying factory equipment. 32 Economic conditions worsened in 1816.
List B Effects
A Troops were sent into the area. B Weavers stopped working at home and went to work in factories. C Rioters often wore disguises. D Workers destroyed factory equipment. E Many rioters were hanged. F Charlotte Bronte wrote a novel about the Luddites. G Prices went up, and salaries went down. H Factory owners did not need to hire skilled weavers. I Luddite rioting resumed for a short while. J People compared Ned Ludd to Robin Hood.
Questions 33—40. Do the following statements agree with the information given in the passage? On lines 33—40 on your answer sheet- write:
TRUE if the statement agrees with the information FALSE if the statement contradicts the information NOT GIVEN if there is no information on this
33 A Luddite is a person who resists new technology. 34 Before the nineteenth century, weavers made lace by hand. 35 Factory owners as well as workers died as a result of Luddite rioting. 36 The Luddite movement did not spread beyond England. 37 Nobody knows for certain who Ned Ludd was. 38 Worker protests during the economic downturn of 1816 were nonviolent. 39 Luddite activity lasted for many years. 40 Neo-Luddites do not use computers.
Do you need printed IELTS/ OET practice material? Place your order today. Available now for just Rs: 1,100 (including shipping all across India) Contact us at our WhatsApp number: +91 9886926773 to place your order. (Free for LTC students)
We hope this information has been valuable to you. If so, please consider a monetary donation to Lifestyle Training Centre via UPI. Your support is greatly appreciated.
Would you like to undergo training for OET, PTE, IELTS, Duolingo, Phonetics, or Spoken English with us? Kindly contact us now!
Do you need printed IELTS/ OET practice material? Place your order today. Available now for just Rs: 1,100 (including shipping all across India) Contact us at our WhatsApp number: +91 9886926773 to place your order. (Free for LTC students)
We hope this information has been valuable to you. If so, please consider a monetary donation to Lifestyle Training Centre via UPI. Your support is greatly appreciated.
Would you like to undergo training for OET, PTE, IELTS, Duolingo, Phonetics, or Spoken English with us? Kindly contact us now!
We hope this information has been valuable to you. If so, please consider a monetary donation to Lifestyle Training Centre via UPI. Your support is greatly appreciated.
Would you like to undergo training for OET, PTE, IELTS, Duolingo, Phonetics, or Spoken English with us? Kindly contact us now!
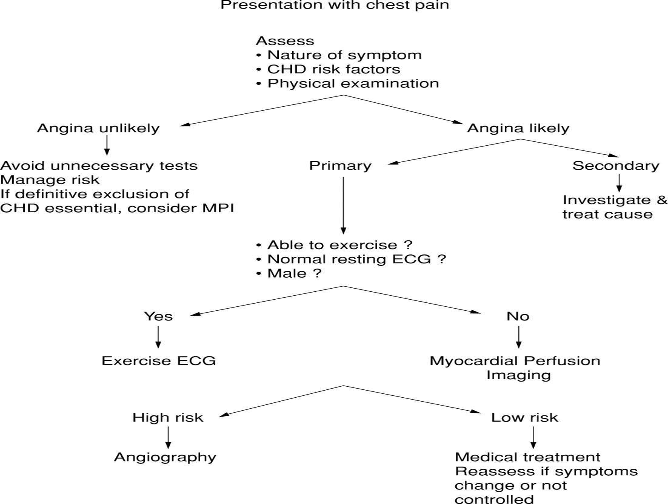
Text A Cardiovascular disease is the leading cause of death in the United States for men and women of all racial and ethnic groups. Angina pectoris is a clinical syndrome usually characterized by episodes or paroxysms of pain or pressure in the anterior chest. The cause is insufficient coronary blood flow, resulting in a decreased oxygen supply when there is increased myocardial demand for oxygen in response to physical exertion or emotional stress.
Text B – Risk factors a. Family history b. Increasing age, particularly women c. Gender: men; women, especially after menopause (estrogen seems to provide some protection) d. Race; risk appears higher in African-Americans e. Cigarette smoking contributes to vasoconstriction, platelet activation, arterial smooth muscle cell proliferation, and reduced oxygen availability f. Hypertension; widened QRS complex (bundle branch block) g. Hyperlipidemia: increased total cholesterol; increased LDL (high: 130 to150 mg/dL; very high: 160 mg/dL or more); increased ratio of total cholesterol or LDL to HDL; low HDL (less than 40 mg/dL); HDL greater than 60 mg/dL seems to help protect against coronary artery disease (CAD); increased triglycerides (high:200 to 499 mg/dL; very high: 500 mg/dL or more) h. Obesity (particularly abdominal obesity) i. Sedentary lifestyle (contributes to obesity and reduced HDL) j. Type 2 diabetes k. Stress; an innate, competitive, aggressive type A personality seems less important than amount of stress and client’s psychologic response) l. Metabolic syndrome: cluster of signs including hyperlipidemia, low HDL level, abdominal obesity, increased BP, insulin resistance, increased levels of C-reactive protein, and increased fibrinogen level Text C
Text D Management of acute MI A. Improvement of perfusion (1) Administration of aspirin immediately (2) Beta blockers or angiotensin II receptor blockers for left ventricular systolic dysfunction (LVSD) (3) Thrombolytic therapy within 30 minutes of arrival; anticoagulants (4) IV nitroglycerin (5) ACEIs (6) Anti-dysrhythmics to maintain cardiac function (7) PCI within 90 minutes of arrival at emergency department (8) Intraaortic balloon pump that inflates during diastole and deflates during systole to decrease cardiac workload by decreasing after load and increasing myocardial perfusion for cardiogenic shock (9) Aspirin, beta blocker, and possible antilipidemic prescribed at discharge B. Promotion of comfort and rest (1) Analgesics (e.g., IV morphine) to reduce pain, anxiety, and cardiac Work load by decreasing preload and after load (2) Oxygen to improve tissue oxygenation (3) Maintenance of bed or chair rest to decrease oxygen tissue demands (4) Diet therapy: 2g sodium diet or clear liquids, depending on presence of nausea
PART A TIME: 15 minutes • Look at the four texts, A – D, in the separate Text Booklet • For each question, 1-20, look through the texts, A-d, to find the relevant information. • Write your answers on the spaces provided in this Question Paper. • Answer all the questions within the 15-minute time limit. ANGINA PECTORIS 1. How to assess chest pain? …………………………………………………………………. 2. The major cause of angina pectoris …………………………………………………….. 3. Metabolic syndrome may also contribute to angina …………….…… 4. It is required to take ECG for patients with chest pain…………………… 5. How acute MI can be managed? ………………………………… 6. Importance of pain medications in management of chest pain…………………. 7. Greater levels of high-density lipoprotein in the body protects from cardiac illness………………
Questions 8-14 Answer each of the questions, 8-4, with a word or short phrase from one of the texts. Each answer may include words, number of the both. Your answers should be correctly spelled. 8. What is the main symptom of angina pectoris? 9. What contributes to obesity and reduced HDL? 10. Which is the leading cause of death in the US for both the genders? 11. What should be administered within half an hour of arrival of client with angina? 12. What should be avoided if the client exhibits chest pain which is angina unlikely? 13. What is recommended in order to reduce oxygen tissue demands? 14. What is the next step involved in the angina assessment protocol, if the client’s resting ECG is normal?
Questions 15-20 Complete each of the sentences, 15- 20, with a word or short phrase from one of the texts. Each answer may include words, number or both. Your answers should be correctly spelled 15. …………………….. should be administered within one and half hour of arrival. 16. Beta blockers or angiotensin II receptor blockers to be administered for………………….. 17. The risk of angina appears higher in………………… 18. ………………………is used to reduce cardiac workload which works by decreasing after load and increasing myocardial perfusion. 19. ……………………….. contributes to vasoconstriction and platelet activation 20. ……………………….. sodium diet or clear liquids are recommended depending on presence of nausea
Part B In this part of the test, there are six short extracts relating to the work of health professionals. For questions 1-6, choose answer (A, B, or C) which you think fits best according to the text.
1) Living will-2 1. According to the paragraph, a living will covers certain situation, except, a. during the need of resuscitation, ventilation and dialysis b. to receive only pain medication c. when there is no life threatening injury is present 1. A living will addresses many of the medical procedures common in life- threatening situations, such as resuscitation via electric shock, ventilation and dialysis. One can choose to allow some of these procedures or none of them. One can also indicate whether he or she wishes to donate his or her organs and tissues after death. Even if he or she refuses life-sustaining care, he or she can express the desire to receive pain medication throughout his or her final hours. In most states, one can extend his or her living will to cover situations where he or she has no brain activity or where doctors expect him or her to remain unconscious for the rest of his or her life, even if a terminal illness or life-threatening injury isn’t present. Because these situations can occur to any person at any age, it’s a good idea for all adults to have a living will.
2. The passage says regarding suprapubic catheter that a. It is better than indwelling catheters b. It is preferred for short-term urinary drainage c. It may cause damage to the urethra, if it is not secured with sutures or tape 2. Suprapubic catheter A suprapubic catheter may be used for long-term continuous urinary drainage. This type of catheter is surgically inserted through a small incision above the pubic area. Suprapubic bladder drainage diverts urine from the urethra when injury, stricture, prostatic obstruction, or gynecologic or abdominal surgery has compromised the flow of urine through the urethra. A suprapubic catheter is often preferred over indwelling urethral catheters for long-term urinary drainage. Suprapubic catheters are associated with decreased risk of contamination with organisms from fecal material, elimination of damage to the urethra, a higher rate of patient satisfaction, and lower risk of catheter-associated urinary tract infections. The drainage tube is secured with sutures or tape. Care of the patient with a suprapubic catheter includes skin care around the insertion site; care of the drainage tubing and drainage bag is the same as for an indwelling catheter.
3. Evaluation of breast cancer by using PET/CT scan a. provides accurate results than the PET scan alone b. to be compared with PET or CT scan alone c. has been receiving no attention because it’s results to be compared with the PET or CT scan alone. 3. The Role of PET/CT for Evaluating Breast Cancer Positron emission tomography combined with computed tomography (PET/CT) has been receiving increasing attention during the recent years for making the diagnosis, for determining the staging and for the follow-up of various malignancies. The PET/CT findings of 58 breast cancer patients (age range: 34 79 years old, mean age: 50 years) were retrospectively compared with the PET or CT scans alone. PET/CT was found to be better than PET or CT alone for detecting small tumors or multiple metastases, for accurately localizing lymph node metastasis and for monitoring the response to chemotherapy in breast cancer patients.
4. The purpose of the guidelines is; a. To conduct competitions in environmental health, between the health care providers regarding management of pediatric asthma b. Merge environmental management of asthma with child health care c. To provide environmental instructions to the patients 4. Extract from “Environmental Management of Pediatric Asthma: Guidelines for Health Care Providers” These guidelines are aimed at integrating environmental management of asthma into pediatric health care. These documents outline competencies in environmental health relevant to pediatric asthma that should be mastered by health care providers, and outlines the environmental interventions that should be communicated to patients. The guidelines contain three components: Competencies (Competencias en Espanol): An outline of the knowledge and skills that health care providers and health professional students should master and demonstrate in order to incorporate management of environmental asthma triggers into pediatric practice. Environmental History Form: A quick, user-friendly document that can be used as an intake tool to help determine pediated patients’ environmental asthma triggers. Environmental Intervention Guidelines: Follow-up questions and intervention solutions to environmental asthma triggers.
5. While dispensing dangerous drugs a. RN must document the preparation and performance time b. RN must follow the written drug dispersing procedure as well as nurse protocol c. Pharmacist and physician may need to sign the procedure 5. Subject: DISPENSING DANGEROUS DRUGS RNs are authorized to dispense dangerous drugs only under the following conditions: The dispensing is in accordance with a written drug dispensing procedure and under the authority of an order issued in conformity with a nurse protocol. There must be documented preparation and performance (i.e., ability to perform) specific to dispensing dangerous drugs based on a written dispensing procedure. Documentation should include that each RN has read and understands the drug dispensing procedure. A copy of the drug dispensing procedure must be accessible in each of the specific settings where RNs dispense under nurse protocols and be available upon request. The procedure must be signed by the pharmacist and physician who have established it.
6. A metabotropic receptors a. form an ion channel pore b. are coupled with G-proteins c. are directly linked with ion channels on the plasma membrane 6.A metabotropic receptor A metabotropic receptor is a type of membrane receptor of eukaryotic cells that acts through a second messenger. It may be located at the surface of the cell or in vesicles. Based on their structural and functional characteristics, the neurotransmitter receptor can be classified into two broad categories: metabotropic and ionotropic receptors. Ionotropic receptors form an ion channel pore. In contrast, metabotropic receptors are indirectly linked with ion channels on the plasma membrane of the cell through signal transduction mechanisms, often G proteins. Hence, G protein-coupled receptors are inherently metabotropic. Other examples of metabotropic receptors include tyrosine kinases and guanylyl cyclase receptors. Both receptor types are activated by specific neurotransmitters. When an ionotropic receptor is activated, it opens a channel that allows ions such as Na+, K+, or Cl− to flow. In contrast, when a metabotropic receptor is activated, a series of intracellular events are triggered that can also result in ion channels opening or other intracellular events, but involve a range of second messenger chemicals
PART C In this part of the test, there are two tests about different aspects of health care. For questions 7 – 22, choose the answer (A, B, C , or D) which you think fits best according to the text
Text 1: Ebola Virus and Marburg Virus
The Ebola virus and Marburg virus are related viruses that cause hemorrhagic fevers — illnesses marked by severe bleeding (hemorrhage), organ failure and, in many cases, death. Both the Ebola virus and Marburg virus are native to Africa, where sporadic outbreaks have occurred for decades.
The Ebola virus and Marburg virus both live in animal hosts, and humans can contract the viruses from infected animals. After the initial transmission, the viruses can spread from person to person through contact with bodily fluids or contaminated needles.
No drug has been approved to treat the Ebola virus or Marburg virus. People diagnosed with the Ebola or Marburg virus receive supportive care and treatment for complications. Scientists are coming closer to developing vaccines for these deadly diseases.
In both the Ebola virus and Marburg virus, signs and symptoms typically begin abruptly within the first five to 10 days of infection. Early signs and symptoms include: fever, severe headaches, joint and muscle aches, chills, sore throat and weakness. Over time, symptoms become increasingly severe and may include: nausea and vomiting, diarrhea (may be bloody), red eyes, raised rash, chest pain and coughing, stomach pain, severe weight loss, bleeding from the nose, mouth, rectum, eyes and ears.
Ebola virus has been found in African monkeys, chimps and other nonhuman primates. A milder strain of Ebola has been discovered in monkeys and pigs in the Philippines. The Marburg virus has been found in monkeys, chimps and fruit bats in Africa.
The virus can be transmitted to humans by exposure to an infected animal’s bodily fluids, including blood. Butchering or eating infected animals can spread the viruses; scientists who have operated on infected animals as part of their research have also contracted the virus.
Infected people typically don’t become contagious until they develop symptoms. Family members are often infected as they care for sick relatives or prepare the dead for burial. Medical personnel can be infected if they don’t use protective gear such as surgical masks and latex gloves. Medical centers in Africa are often so poor that they must reuse needles and syringes and some of the worst Ebola epidemics have occurred because contaminated injection equipment wasn’t sterilized between uses. There’s no evidence that the Ebola virus or Marburg virus can be spread via insect bites.
Ebola and Marburg hemorrhagic fevers are difficult to diagnose because many of the early signs and symptoms resemble those of other infectious diseases, such as typhoid and malaria. But if doctors suspect that you have been exposed to the Ebola virus or Marburg virus, they use laboratory tests that can identify the viruses within a few days.
Most people with Ebola or Marburg hemorrhagic fever have high concentrations of the virus in their blood. Blood tests known as enzyme-linked immunosorbent assay ’(ELISA)’ and reverse transcriptase polymerase chain reaction ‘(PCR)’ can detect specific genes or the virus or antibodies to them.
No antiviral medications have proved effective in treating Ebola virus or Marburg virus infection. As a result, treatment consists of supportive hospital care. This includes providing fluids, maintaining adequate blood pressure, replacing blood loss and treating any other infections that develop.
As with other infectious diseases, one of the most important preventive measures for Ebola virus and Marburg virus is frequent hand-washing. Use soap and water, or use alcohol-based hand rubs containing at least 60 percent alcohol when soap and water aren’t available. In developing countries, wild animals, including nonhuman primates, are sold in local markets. Avoid buying or eating any of these animals.
In particular, caregivers should avoid contact with the person’s body fluids and tissues, including blood, semen, vaginal secretions and saliva. People with Ebola or Marburg are most contagious in the later stages of the disease.
If you’re a health care worker, wear protective clothing — such as gloves, masks, gowns and eye shields. Keep infected people isolated from others. Carefully disinfect and dispose of needles and other instruments. Injection needles and syringes should not be reused.
Scientists are working on a variety of vaccines that would protect people from Ebola or Marburg viruses. Some of the results have been promising, but further testing is needed.
Text 1: Questions 7-14
7. The Ebola and Marburg Viruses are native to A. America B. Japan C . Africa D. China
8. According to the passage(s), the Ebola and Marburg viruses A. spread from person to person only B. spread from animals to humans C. spread from animals to animals D. spread person to person after initial transmission from the infected animals
9. One of these statements is true, according to the information given in the passage(s) A. scientists have developed vaccines for the treatment of Ebola and Marburg diseases B. scientists are closer to developing an effective vaccine for the treatment C. it is not possible to fight the diseases caused by Ebola and Marburg D. scientists have discovered the causes of the transmission of the viruses from animal to human
10. Symptoms are typically seen within A. five days B. ten days C. five to seven days D. five to ten days
11. In the Philippines, Ebola was discovered in A. chimpanzees B. human primates C. non-human primates D. monkeys
12. Most known Ebola diseases occur due to A. contamination B. bodily fluids C. contaminated needles and syringes D. none
13. People with hemorrhagic fever show A. high number of viruses in their blood B. low concentrations of virus C. high concentrations of antibodies D. low concentrations of antibodies
10. As a health care worker, you A. should keep infected people totally isolated from others B. should not reuse needles and syringes for the second time C. should wear clothing such as gowns and eye shields D. none of the above
PART C Text 2: A Chronic Disease – Atopic Dermatitis
Atopic dermatitis is a common chronic skin disease. It is also called atopic eczema. ‘Atopic’ is a term used to describe allergic conditions such as asthma and hay fever. Both dermatitis and eczema mean inflammation of the skin. People with atopic dermatitis tend to have dry, itchy and easily irritated skin. They may have times when their skin is clear and other times when they have rash.
In infants and small children, the rash is often present on the skin around the knees and elbows and the cheeks. In teenagers and adults, the rash is often present in the creases of the wrists, elbows, knees or ankles, and on the face or neck.
Atopic dermatitis usually begins and ends during childhood, but some people continue to have the disease into adulthood. If you have ever had atopic dermatitis, you may have trouble with one or more of these: dry, sensitive skin, hand dermatitis and skin infections.
The exact cause of atopic dermatitis is unknown. Research suggests that atopic dermatitis and other atopic diseases are genetically determined; this means that you are more likely to have atopic dermatitis, food allergies, asthma and/or hay fever if your parents or other family members have ever had atopic dermatitis. These diseases may develop one after another over a period of years. This is called the ―atopic march.
Recognizing that a person with atopic dermatitis is at a higher risk of developing one of these diseases is important for parents, patients and health care providers. Knowing that a child with a slight wheeze has had a history of atopic dermatitis, for example makes it easier to diagnose the subtle onset of asthma. There are many things that make the itching and rash of atopic dermatitis worse. When you learn more about atopic dermatitis and how to avoid things that make it worse, you may be able to lead a healthier life.
If you have a reaction to something you touch, breathe or eat, you might have an allergy. Allergies can trigger or worsen your atopic dermatitis symptoms. Common causes of allergy are: dust mites, furry and feathered animals, cockroaches, pollen, mold, foods, chemicals.
Your health care provider may recommend allergy testing and food challenges to see if allergies worsen itching or rashes. Allergy testing may include skin testing, blood tests or patch tests. Many measures can be taken to avoid things to which you are allergic. Although many of the measures can be done for the entire home, the bedroom is the most important room to make skin friendly. Talking with health care provider about what measures you can take to avoid your allergens can be very beneficial.
Food allergies may be the cause of itching or rashes that occur immediately after eating, especially in children. Some common food allergens include milk, eggs, peanuts, wheat, nuts, soy and seafood. Most people are allergic to only one, two or at the most three foods. Be aware that diet restrictions can lead to poor nutrition and growth delay in babies and children. Talk with your health care provider about maintaining a well-balanced diet.
Emotions and stress do not cause atopic dermatitis, but they may bring on itching and scratching. Anger, frustration and embarrassment can cause flushing and itching. Day to day stresses as well as major stressful events can lead to or worsen the itch-scratch cycle. The medications used in atopic dermatitis include: Topical steroids, Topical immuno modulators, Tar products, Antiinfectives, Antihistamines.
Steroid medicines that are applied to the skin are called topical steroids. Topical steroids are drugs that fight inflammation. They are very helpful when rash is not well controlled. Topical steroids are available in many forms such as ointments, creams, lotions and gels. It is important to know that topical steroids are made in low to super potent strengths. Steroid pills or liquids, like prednisone, should be avoided because of side effects and because the rash often comes back after they are stopped.
Text 2: Questions 15 to 22
15. People with atopic dermatitis suffer from A. hay fever B. asthma C. dry, itchy and irritated skin D. rashes 16. In small children, a rash is seen A. around elbows B. on the face C. on the neck D. around the knees 17. People with atopic dermatitis have A. dry skin B. skin infections C. hand dermatitis D. all of the above 18. The term atopic in the passage 1 refers to A. allergic diseases B. asthma and hay fever C. allergic conditions like hay fever D. allergic conditions like asthma 19. can worsen dermatitis symptoms A. allergies B. pollen C. dust D. mold 20. According to the information given in the passage(s), avoiding allergens is A. easy B. difficult C. sometimes easy and sometimes difficult D. can’t say 21. Allergic conditions like asthma in patients who have had a history of atopic dermatitis can be easily diagnosed by health professionals, this statement is A. out of the paragraphs given B. false C. true D. can be true or can be false 22. According to information given, common food allergens can be in A. milk, egg, fish B. fish, nuts, soya been C. nuts, eggs, wheat D. milk, cereals, sea food
We hope this information has been valuable to you. If so, please consider a monetary donation to Lifestyle Training Centre via UPI. Your support is greatly appreciated.
Would you like to undergo training for OET, PTE, IELTS, Duolingo, Phonetics, or Spoken English with us? Kindly contact us now!
We hope this information has been valuable to you. If so, please consider a monetary donation to Lifestyle Training Centre via UPI. Your support is greatly appreciated.
Would you like to undergo training for OET, PTE, IELTS, Duolingo, Phonetics, or Spoken English with us? Kindly contact us now!
We hope this information has been valuable to you. If so, please consider a monetary donation to Lifestyle Training Centre via UPI. Your support is greatly appreciated.
Would you like to undergo training for OET, PTE, IELTS, Duolingo, Phonetics, or Spoken English with us? Kindly contact us now!