We hope this information has been valuable to you. If so, please consider a monetary donation to Lifestyle Training Centre via UPI. Your support is greatly appreciated.
Would you like to undergo training for OET, PTE, IELTS, Duolingo, Phonetics, or Spoken English with us? Kindly contact us now!
NF is a rare but serious bacterial infection that affects the tissue beneath the skin, and surrounding muscles and organs (fascia). It is often called the “flesh-eating disease”, although the bacteria that cause it don’t “eat” flesh – they release toxins that damage nearby tissue. NF is caused by bacteria that gain access to the body, often from only a relatively minor injury, such as a small cut. The conditions gets worse very quickly and can be life threatening if it’s not recognised and treated early on. Around a quarter of patients with NF will die of their infection, but this varies with the severity of the infection and the underlying health of the patient. Quite a few different types of bacteria can cause the disease. However, when they cause infection elsewhere, many are only associated with mild disease. These include group A streptococci, a common cause of tonsillitis, and Clostridium perfringens, a cause of food poisoning. The infection can also be spread from person to person, but this is very rare. About 400 cases of NF are diagnosed in Australian hospitals each year, which is similar to the incidence reported in other countries. Anyone can get necrotising fasciitis, including young and otherwise healthy people. It tends to affect older people and those in poor general health
TEXT 2: Contracting necrotising fasciitis
For a person to develop necrotising fasciitis, several factors relating to themselves, the environment and the presence of certain bacteria all have to be present. •Patient factors that increase their risk if exposed to bacteria include: -impaired immunity -obesity -acne or asthma sufferers -chronic diseases such as diabetes, peripheral vascular disease -a breach of the skin such as: – surgical wounds – accidental wounds – intravenous drug use •Environmental factors that increase risk include: -coral cuts in marine environments -contaminated surgical environment or equipment -contamination of intra venous injected substances •Bacteria that can lead to issues include: -Group A streptococci are commonly found in the throat and on the skin and is the most common bacteria to cause NF -Vibrio bacteria are gram-negative bacteria that grow well in salty environments -Aeromonas are Gram-negative, anaerobic bacteria that occur in aquatic environments – Cleansing wounds, keeping wound covered and good hand hygiene are the main ways to prevent necrotising fasciitis
TEXT 3: Symptoms of necrotising fasciitis
The symptoms of NF develop quickly over hours or days. They may not be obvious at first and can be similar to less serious conditions such as flu, gastroenteritis or cellulitis. It might take 3 or 4 days for symptoms to fully appear. Skin becoming red, hot and blistered, together with the patient reporting intense pain in the infected area are the main early symptoms. Patients with NF report pain that is out of proportion to the changes in skin condition. This is a key warning sign. The pain remains intense until the necrosis kills the nerve endings. Other symptoms include: -oedema, or swelling -crackling under the skin -confusion -dehydration -diarrhoea and vomiting -skin swells and changes colour, turning violet -areas of tissue turn black and start to die After 4 or 5 days, septicaemia is likely to develop causing high temperature, dangerously low blood pressure, and they possible loss of consciousness. Without treatment, necrotizing fasciitis is always fatal.
TEXT 4: Treatment and outlook:
NF needs to be treated in hospital, usually in the intensive care unit The main treatments are: •surgery to remove infected tissue which may repeated several times to ensure all the infected tissue is removed, and occasionally it may be necessary to amputate affected limbs •antibiotics, usually several different types, administered intravenously •supportive treatment of blood pressure, fluid levels and organ functions- People usually need to stay in hospital for several weeks. NF can progress very quickly and lead to serious problems such as blood poisoning (sepsis) and organ failure and even with treatment, it is estimated that 1 or 2 in every 5 cases are fatal. People who survive the infection are sometimes left with long-term disability as a result of amputation or the removal of a lot of infected tissue. They may need further surgery to improve the appearance of the affected area and may need ongoing rehabilitation support to help them adapt to their disability.
Questions 1-7 For each question, 1-7, decide which text (A, B, C or D) the information comes from. You may use any letter more than once. In which text can you find information about
1 What conditions can develop in a person with blood poisoning? _________________ 2 Ways to stop develop necrotising fasciitis? _________________ 3 The prognosis for people with necrotising fasciitis? _________________ 4 The preponderance of necrotising fasciitis diagnosed in Australian hospitals? __________ 5 Underlying issues that can make person more susceptible to developing NF? __________ 6 Operations that can be done to treat necrotising fasciitis? _________________ 7 The timeframe for symptoms of NF to be full blown? _____________
Questions 8-14. Answer each of the questions, 8-14, with a word or short phrase from one of the texts. Each answer may include words, numbers or both.
8 What types of lesions may let bacteria invade the body? _________________ 9 What type of pain in the infected area do patients experience? _________________ 10 What type of infection is necrotising fasciitis? _________________ 11 Which bacteria is most likely to lead to NF? _________________ 12 Which part of a hospital are people with necrotising fasciitis usually treated? _________________ 13 What might a person cut themselves on in an ocean that could lead to them getting necrotising fasciitis? 14 For every 5 people with necrotising fasciitis, how many are likely to die, even with treatment_______
Questions 15-20 Complete each of the sentences, 15-20, with a word or short phrase from one of the texts. Each answer may include words, numbers or both.
15 People with necrotising fasciitis say their pain is_________________ to what can be seen in the area. 16 Symptoms of NF might be vague at first and more like common conditions such as_________________or cellulitis. 17 People who have conditions such as: _________________obesity and acne or asthma have a greater chance of developing NF if they are exposed to Group A streptococci bacteria. 18 Often multiple antibiotics are_________________to treat NF. 19 NF is more likely to be a problem for_________________and those in poor general health. 20 NF is commonly known as the_________________
PART B TEXT 1:
Know the Difference: Infiltration vs. Extravasation Intravenous infiltration is one of the most common problems that can occur when fluid infuses into the tissues surrounding the venepuncture site. This sometimes happens when the tip of the catheter slips out of the vein or the catheter passes through the wall of the vein. If you are concerned an IV is infiltrated, standard procedures should be followed by, for example, discontinuing the site and relocating the IV. Know the Difference: Infiltration vs. Extravasation An extravasation occurs when there is accidental infiltration of a vesicant or chemotherapeutic drug into the surrounding intravenous site. Vesicants can cause tissue destruction and / or blistering. Irritants can result in pain at the site and along the vein and may cause inflammation. The treatment for extravasation will vary depending on hospital policy. Question 1) What should you do if you think an IV is infiltrated? a) You should terminate the procedure before trying again b) You should change the catheter c) You should irrigate the surrounding intravenous site
TEXT 2 : Arterial Line Placement Arterial line placement is a common procedure in various critical care settings. Intra-arterial blood pressure measurement is more accurate than measurement by non-invasive means, especially in the critically ill. Intra-arterial blood pressure management permits the rapid recognition of changes that is vital for patients on continuous infusions of vasoactive drugs. Overall, arterial line placement is considered a safe procedure, with a rate of major complications that is below 1%. Arterial Line Placement In both adults and children, the most common site of cannulation is the radial artery, primarily because of the superficial nature of the vessel and the ease with which the site can be maintained. Additional advantages of radial artery cannulation include the consistency of the anatomy and the low rate of complications. Question 2) Why is the radial artery usually chosen for cannulation? a) its low profile anatomy is ideal for primary cannulation b) the site can be maintained during other non-invasive manipulations c) it has a shallow position
TEXT 3: Clinically Important Symptoms of PTSD People with clinically important symptoms of PTSD (Post-Traumatic Stress Disorder) refer to those who are assessed as having PTSD on a validated scale, as indicated by baseline scores above clinical threshold, but who do not necessarily have a diagnosis of PTSD. They are typically referred to in studies that have not used a clinical interview to arrive at a formal diagnosis of PTSD and instead have only used self-report measures of PTSD symptoms. Complex PTSD develops in a subset of people with PTSD. It can arise after exposure to an event or series of events of an extremely threatening or horrific nature, most commonly prolonged or repetitive events from which escape is difficult or impossible. The disorder is characterised by the core symptoms of PTSD; that is, all diagnostic requirements for PTSD are met. Question 3) According to this article, people with PTSD a) have a high score on a validated scale, which includes complex PTSD factors b) have experienced prolonged or repetitive symptoms c) have not been examined by qualified clinicians
TEXT 4 How to Assess a Peripheral Intravenous Cannula: Most patients need at least one peripheral intravenous cannula during their hospital stay for intravenous fluids and medications, blood products or nutrition. Complications are common but they can be prevented or minimised by routine assessment. Explanations to patients should be provided, along with education about the treatment. Ensure the patient knows why the treatment is being given, and encourage them to speak up if there are any problems, such as pain, leaking, swelling, etc. The cannula should not be painful. Pain is an early symptom of phlebitis (inflammation of the vein) and could indicate that the cannula is not working well and should be removed. Involving the patient and their family empowers them to voice their concerns, and prompts nurses to address problems and remove Question 4) According to this article, patients experiencing pain at the cannula site should a) tell someone b) ask for medication to stop leaking and/or swelling c) remove the cannula in order to avoid phlebitis (inflammation of the vein)
TEXT 5. Japan Approves New Cell Therapy Trial for Spinal Cord Injury The Japanese government’s health ministry has given the go-ahead for a trial of human induced stem cells to treat spinal cord injury. The treatment will be tested in a handful of patients who suffered nerve damage in sports or traffic accidents. Researchers at Osaka University plan to recruit adults who have sustained recent nerve damage in sports or traffic accidents. The team’s intervention involves removing differentiated cells from patients and ‘reprogramming’ them into neural cells. Clinicians will then inject about two million of these cells into each patient’s site of injury. The approach has been successfully tested in a monkey, which recovered the ability to walk after paralysis. These tests follow researcher carried out at Kyoto University which used cells to treat Parkinson’s disease Question 5) How many people will be involved in the trial? a) around two million b) as many patients as possible c) less than ten
TEXT 6 Steroid Nasal Sprays and Drops A steroid nasal spray usually works well to clear all the nasal symptoms such as itching or sneezing. It works by reducing inflammation in the nose. A steroid nasal spray also tends to ease eye symptoms although it is not clear how this occurs. However, they can take up to several days to build up to the full effect. Steroid nasal sprays should be used each day over the hay fever season to keep symptoms away. However, once symptoms have gone, the amount of steroid spray can often be reduced to a low maintenance dose each day to keep symptoms manageable. Side-effects or problems with steroid nasal sprays are rare. Question 6) How long can a nasal spray be used? a) While symptoms such as itching or sneezing occur and after b) Before and during the time symptoms occur c) Before, during the time symptoms occur and after
PART C TEXT 1 Heat and ice have been used for many years to treat pain and to reduce swelling, and many people have found them effective. More recently, studies have been done to investigate whether heat and ice really make a difference to healing and the results have been inconclusive. In general, when used sensibly, they are safe treatments which make people feel better and have some effect on pain levels and there are few harms associated with their use.
Heat is an effective and safe treatment for most aches and pains. Heat can be applied in the form of a wheat bag, heat pads, deep heat cream, hot water bottle or heat lamp. Heat causes the blood vessels to open wide (dilate). This brings more blood into the area to stimulate healing of damaged tissues. It has a direct soothing effect and helps to relieve pain and spasm. It can also ease stiffness by making the tissues more supple. If heat is applied to the skin, it should not be hot; gentle warmth will be enough. If excessive heat is applied there is a risk of burns and scalds. A towel can be placed between the heat source and the skin for protection. The skin must be checked at regular intervals.
Heat should not be used on a new injury. It will increase bleeding under the skin around the injured area and may make the problem worse. The exception to this is new-onset low back strains. A lot of the pain in this case is caused by muscle spasm rather than tissue damage, so heat is often helpful. A large-scale study suggested that heat treatment had a small helpful effect on how long pain and other symptoms go on for in short-term back pain. This effect was greater when heat treatment was combined with exercise.
Ice has traditionally been used to treat soft tissue injuries where there is swelling. However, there is a growing body of evidence which suggests that applying ice packs to most injuries does not contribute to recovery and may even prolong recovery. This is related to the fact that reducing the temperature at the site of an injury will delay the body’s immune system response. It is the action of the immune system which will heal the injury. In one study, some people who used ice said that it was helpful for managing pain, although this did not translate into a lower use of painkillers. Many people find that ice is helpful when used to manage pain in the short term. It is unlikely that it will have much of a negative effect in the long term when used in this way.
A review of studies into the effectiveness of ice treatment found that most studies were inconclusive and others showed only a small effect. For example, a review of studies using hot and cold therapy for osteoarthritis of the knee found that ice packs reduced swelling and that ice massage improved muscle strength and range of movement. Heat packs had no effect on pain and swelling. No side-effects were reported to either heat or ice. Another study, which looked at a variety of treatments for neck pain, found that neither heat nor cold was effective.
In the later, or rehabilitation, phase of recovery the aim changes to restoring normal function. At this stage the effects of ice can enhance other treatments, such as exercise, by reducing pain and muscle spasm. This then allows better movement. If you are doing exercises as part of your treatment, it can be useful to apply an ice pack before exercise. This is so that after the ice pack is removed the area will still be a little numb. The exercises can also be done with the ice pack in place. This reduces pain and makes movement around the injury more comfortable, although it can also make the muscles being exercised stiffer.
Ice packs can be made from ice cubes in a plastic bag or wet tea towel. A packet of frozen peas is also ideal and can be used very easily. These mould nicely and can go in and out of the freezer. However, frozen vegetables should not be eaten if they have been thawed and re-frozen. Purpose-made cold packs can also be bought from pharmacies. Take care when using ice and cold packs from a deep freeze, as they can cause ice burns quickly if used without care and proper protection.
Ideally, ice should be applied within 5-10 minutes of injury and for 20-30 minutes. This can be repeated every 2-3 hours or so whilst you are awake for the next 24-48 hours. Do not use ice packs on the left shoulder if you have a heart condition. Do not use ice packs around the front or side of the neck. Both heat and ice can be re-applied after an hour if needed.
Questions 7-14 7) What have studies shown about heat and ice treatments? a) Results show heat and ice really make a difference b) Results are uncertain c) Results have not been investigated d) Results show they can cause harm
8) What do we learn about heat in the second paragraph? a) it increases muscle tissue b) it provokes tissue stiffness c) it changes the behaviour of the blood flow d) it can cause muscle spasm
9) What did the study mentioned in the third paragraph find? a) heat made a problem worse b) heat triggered muscle spasms c) heat increased new-onset low back pain d) heat changed the duration of back pain
10) In the fourth paragraph, what have results shown concerning the use of ice? a) Ice could lengthen the time it takes to improve b) Ice stimulates the body’s immune response c) Using ice therapies reduces the need for painkillers d) Ice causes swelling in soft tissue injuries
11) In the fifth paragraph, the review found that a) heat packs had some small side-effects b) ice massage had a positive effect on some muscles c) heat therapy worked best on cases of osteoarthritis of the knee d) heat treatment was more effective than ice treatment
12) In the sixth paragraph, what positive effect of using ice packs is described? a) they eliminate the need for other treatments b) they make some areas less sensitive to pain c) they move the pain to a different area d) they restore normal functions to injured muscles
13) In the seventh paragraph, what does the word ‘these’ refer to? a) frozen peas b) ice cubes c) wet tea towels d) ice packs
14) How long can ice be applied to an injury? a) for five to ten minutes b) no more than half an hour c) for two to three hours d) for 24 to 48 hours
PART C. TEXT 2:
We consider low-dose aspirin so innocuous that we call it baby aspirin. Though we don’t give it to kids anymore, many adults take it every day (at the recommendation of their doctor) to stave off heart attacks and strokes. But just as we now know not to give babies aspirin, expert opinion has shifted on low-dose aspirin for adults, too. Research in the last few years has made it clear that daily aspirin doesn’t help many of the people taking it. If anything, it might hurt them.
New guidelines from the American College of Cardiology (ACC) and the American Heart Association (AHA) say that aspirin, and even baby aspirin should no longer be prescribed. These principles are largely in line with how other major organizations have begun to view aspirin. The 2016 European guidelines on cardiovascular disease prevention don’t recommend it as a primary method of heart attacks or stroke prevention, and the U.S. Preventive Services Task Force recommends it only for people in their 50’s with elevated cardiovascular disease risk. For the rest of the population, it wasn’t clear whether there was a worthwhile benefit.
Aspirin is an antiplatelet drug, which means it prevents blood from clotting as easily. Forming a blood clot is, of course, a crucial capability—if you couldn’t clot at all, you’d bleed out from small wounds. But clots that form inside your blood vessels can block flow entirely, causing a heart attack when that blood fails to get back to your heart, or a stroke if the clot cuts off blood to part of your brain. In theory, preventing platelets from doing their job means aspirin should help decrease the risk of both of these problems. And that’s true, but only for a select group of people.
The new guidelines note that aspirin is still very much recommended as a secondary treatment, meaning it definitely helps people who have already had a heart attack or stroke. These people are at a significantly higher risk of having another incident, and aspirin can reduce that risk. What physicians are no longer recommending is its widespread use as a primary treatment, for people who have never had a heart attack or stroke before. In other words, if you’ve never had a heart attack, you probably shouldn’t consider it.
So-called baby aspirin may carry a low dose, but patients shouldn’t assume that taking it is harmless. Taking a drug that makes your blood less likely to clot puts you at risk. If you start bleeding in your intestines or your brain, for instance, your platelets are supposed to come to the rescue. If you’re on daily aspirin, that happens less effectively. A 2009 study in The Lancet found that there was a small, but not insignificant increased risk of major bleeds amongst people taking aspirin regularly. A 2016 study found the same thing, as did a 2018 study in The New England Journal of Medicine. Those same risks exist if you’ve had a heart attack already, but the benefits you get from taking aspirin start to outweigh the potential downsides once you’re in this category. That trade-off is what the ACC/AHA cite in their revised recommendations. Once your elevated risk of having a heart attack goes over 10 percent, the guidelines note, it becomes favourable to prescribe aspirin daily. That goes for anyone between 40 and 70. There’s not enough evidence in people younger than 40, and adults over 70 have such elevated risk of bleeding that most wouldn’t do well on daily aspirin regardless of cardiac risk.
The overarching advice for everyone, though, is to discuss with your doctor whether you should take low-dose aspirin before deciding to do so (or deciding to stop). These guidelines note that there are likely to be exceptions, and your physician should be assessing your personal health risks when deciding whether to prescribe daily aspirin. This isn’t actually all that new. Though research from the mid-20th century suggested aspirin would help everyone, these changes to official recommendations are based on many years of modern studies, which the ACC/AHA note are far better designed and more rigorous than anything we’ve had before. If your doctor scoffs and tells you baby aspirin is a great idea for everyone of a certain age, their knowledge is out of date.
Reversals in expert opinion are, unfortunately, inevitable—it’s the scientific process at work. Think of it less as flip-flopping and more as a correction to a formerly mistaken belief. And please talk to your doctor before you prescribe yourself baby aspirin.
Questions 15-22 15) The first paragraph informs us that a) even babies can have aspirin b) the viewpoint of experts has changed regarding aspirin c) aspirin can cause strokes d) aspirin dosage depends on doctors’ recommendations
16) According to the second paragraph, the European guidelines a) continue to recommend the use of aspirin b) harmonize with the American guidelines c) recommend aspirin for people in their 50’s d) say that aspirin should not be prescribed to babies
17) The third paragraph informs us that aspirin a) inhibits blood clotting b) helps to heal small wounds c) decreases the production of platelets d) slows bleeding by stimulating clotting
18) What does the last word of the fourth paragraph refer to? a) primary treatment b) secondary treatment c) aspirin d) the new guidelines
19) The 2009 study published in ‘The Lancet’ found a) that aspirin could be a factor in intestinal bleeding b) risks that were different to the study in ‘The New England Journal of Medicine’ c) daily doses of aspirin were less effective d) that the risk of major bleeds was relevant
20) The revised recommendations in the fifth paragraph are a) people younger than 40 should take aspirin b) people older than 70 can take aspirin to elevate risks c) it’s a good idea for middle aged people to take aspirin if they have a higher risk of heart attack d) anyone with a high risk of heart attack should take aspirin
21) What do we learn in the sixth paragraph about modern studies? a) they are superior to older studies b) they confirm earlier studies about the use of aspirin c) they quickly become out of date d) they reveal data that doctors don’t accept
22) In the last paragraph, what does the writer infer about expert opinion? a) experts shouldn’t keep changing their opinions b) changes in opinion are unavoidable c) opinions need to be corrected d) some opinions are unscientific
We hope this information has been valuable to you. If so, please consider a monetary donation to Lifestyle Training Centre via UPI. Your support is greatly appreciated.
Would you like to undergo training for OET, PTE, IELTS, Duolingo, Phonetics, or Spoken English with us? Kindly contact us now!
We hope this information has been valuable to you. If so, please consider a monetary donation to Lifestyle Training Centre via UPI. Your support is greatly appreciated.
Would you like to undergo training for OET, PTE, IELTS, Duolingo, Phonetics, or Spoken English with us? Kindly contact us now!
It helps to remind patients that ADHD is not all bad. ADHD is associated with positive attributes such as being more spontaneous and adventurous. Some studies have indicated that people with ADHD may be better equipped for lateral thinking. It has been suggested that explorers or entrepreneurs are more likely to have ADHD. In addition, GPs can reinforce the importance of developing healthy sleep–wake behaviours, obtaining adequate exercise and good nutrition. These are the building blocks on which other treatment is based. For patients who are taking stimulant medication, it is helpful if the GP continues to monitor their blood pressure, given that stimulant medication may cause elevation. Once a patient has been stabilised on medication for ADHD, the psychiatrist may refer the patient back to the GP for ongoing prescribing in line with state-based guidelines. However, in most states and territories, the GP is not granted permission to alter the dose.
Text B: ADHD: Overview:
Contrary to common belief, ADHD is not just a disorder of childhood. At least 40 to 50% of children with ADHD will continue to meet criteria in adulthood, with ADHD affecting about one in 20 adults. ADHD can be masked by many comorbid disorders that GPs are typically good at recognising such as depression, anxiety and substance use. In patients with underlying ADHD, the attentional, hyperactive or organisational problems pre-date the comorbid disorders and are not episodic as the comorbid disorders may be. GPs are encouraged to ask whether the complaints are of recent onset or longstanding. Collateral history can be helpful for developing a timeline of symptoms (e.g. parent or partner interview). Diagnosis of underlying ADHD in these patients will significantly improve their treatment outcomes, general health and quality of life.
Text C: TABLE 2: Medications for attention deficit hyperactivity disorder and typical dosing
Immediate-release methylphenidate
5 to 10 mg in the morning the first day; add a second dose of 5 to 10 mg at lunch time for a week; then add further increments weekly
Total dose typically varies between 10 mg/day and 60 mg/day Doses of more than 80 mg/day are uncommon (maximum recommended dose in the NICE guidelines is 100 mg/day) 11 Transition to longer-acting formulations can occur after a month
Extended-release methylphenidate
18 or 36 mg/day taken once daily in the morning
Increase in 18 mg increments to a maximum of 72 mg/day Adjust dosage at weekly intervals
Long-acting methylphenidate
20 mg/day taken once daily in the morning
At dose wey in Dose usually would not exceed 60 mg/day
Dexamfetamine
2.5 to 5.0mg in the morning the first day; add a second dose of 2.5 to 5.0mg at lunch time for a week; then add further increments weekly
Total dose typically varies between 5 mg/day and 30 mg/day Doses over 40 mg/day are uncommon (maximum recommended dose in the NICE guidelines is 60 mg/day)11
Lisdexamfetamine
30 mg in the morning the first day; increase up to 70 mg according to response
Dose range typically 30 to 70 mg/ day
Atomoxetine
For those weighing less than 70 kg, start at 0.5 mg/kg taken once daily for three days then increase to 1.2 mg/kg once daily in the morning or as evenly divided doses in the morning and late afternoon/early evening. For those weighing more than 70kg, start at 40 mg/day taken once daily for three days then increase to target dose of 80 mga
Target dose 80 mg/day Maximum dose 100 mg
Text D: Treatment of ADHD
It is very important that the dosage of medication is individually optimised. An analogy may be made
with getting the right pair of glasses – you need the right prescription for your particular presentation with not too much correction and not too little. The optimal dose typically requires careful titration by a psychiatrist with ADHD expertise. Multiple follow-up appointments are usually required to maximise the treatment outcome. It is essential that the benefits of treatment outweigh any negative effects. Common side effects of stimulant medication may include:
• appetite suppression
• insomnia
• palpitations and increased heart rate
• feelings of anxiety
• dry mouth and sweating
In which text can you find information about…
1 different types of ADHD medication? __________
2 possible side effects of medication? ___________
3 conditions which may be present alongside ADHD? _____________
4 a doctor’s control over a patient’s medication? ____________
5 positive perspectives on having ADHD? ___________
6 when patients should take their ADHD medicine? _______________
7 figuring out a patient’s optimal dosage of medication? ________________
Answer each of the questions, 8-14, with a word or short phrase from one of the texts. Each answer may
include words, numbers or both. Your answers should be correctly spelled.
8 What is the maximum recommended dose of Dexamfetamine?
9 What is typically needed to get the best results from ADHD treatment?
10 How can GP’s collect information about their patient’s collateral history?
11 What causes symptoms such as palpitations and anxiety in some patients?
12 What proportion of children with ADHD will carry symptoms into adulthood?
13 What positive personality traits are sometimes associated with ADHD?
14 Which medication has dose recommendations related to patient weight?
Questions 15-20. Complete each of the sentences, 15-20, with a word or short phrase.
Sleep, exercise and nutrition comprise the (15) _______________of further ADHD treatment.
When diagnosing ADHD, it is important to ask if the issues arose recently or are (16) ____________
It is possible to move to (17) ______after one month of immediate-release methylphenidate.
Signs of ADHD can be disguised by (18) _________________ which GPs are more likely to recognise.
GPs should regularly check the (19) _________________ of patients prescribed stimulant medication.
Establishing the ideal dose of ADHD medication needs (20) ________ by an expert psychiatrist.
We hope this information has been valuable to you. If so, please consider a monetary donation to Lifestyle Training Centre via UPI. Your support is greatly appreciated.
Would you like to undergo training for OET, PTE, IELTS, Duolingo, Phonetics, or Spoken English with us? Kindly contact us now!
We hope this information has been valuable to you. If so, please consider a monetary donation to Lifestyle Training Centre via UPI. Your support is greatly appreciated.
Would you like to undergo training for OET, PTE, IELTS, Duolingo, Phonetics, or Spoken English with us? Kindly contact us now!
1. the risks of feeding a child via a nasogastric tube? 2. calculating the length of tube that will be required for a patient? 3. when alternative forms of feeding may be more appropriate than nasogastric? 4. who to consult over a patient’s liquid food requirements? 5. the outward appearance of the tubes? 6. knowing when it is safe to go ahead with the use of a tube for feeding? 7. how regularly different kinds of tubes need replacing?
Questions 8-15. Answer each of the questions, 8-15, with a word or short phrase from one of the texts. Each answer may include words, numbers or both.
8. What type of tube should you use for patients who need nasogastric feeding for an extended period? 9. What should you apply to a feeding tube to make it easier to insert? 10. What should you use to keep the tube in place temporarily? 11. What equipment should you use initially to aspirate a feeding tube? 12. If initial aspiration of the feeding tube is unsuccessful, how long should you wait before trying again? 13. How should you position a patient during a second attempt to obtain aspirate? 14. If aspirate exceeds pH 5.5, where should you take the patient to confirm the position of the tube? 15. What device allows for the delivery of feeds via the small bowel?
Questions 16-20. Complete each of the sentences, 16-20, with a word or short phrase from one of the texts. Each answer may include words, numbers or both. 16. If a feeding tube isn’t straight when you unwrap it, you should it. 17. Patients are more likely to experience long-term feeding via a tube. 18. If you need to give the patient a standard liquid feed, the tube to use is in size. 19. You must take out the feeding tube at once if the patient is coughing badly or is experiencing 20. If a child is receiving ___________ via a feeding tube, you should replace the feed bottle after four hours.
Text A
Paediatric nasogastric tube use Nasogastric is the most common route for enteral feeding. It is particularly useful in the short term, and when it is necessary to avoid a surgical procedure to insert a gastrostomy device. However, in the long term, gastrostomy feeding may be more suitable. Issues associated with paediatric nasogastric tube feeding include: • The procedure for inserting the tube is traumatic for the majority of children. • The tube ls very noticeable. • Patients are likely to pull out the tube making regular re-insertion necessary. • Aspiration, if the tube is incorrectly placed. • Increased risk of gastro-esophageal reflux with prolonged use. • Damage to the skin on the face.
Text B
Inserting the nasogastric tube All tubes must be radio opaque throughout their length and have externally visible markings. 1. Wide bore: – for short-term use only. – should be changed every seven days. – range of sizes for paediatric use is 6 Fr to 10 Fr. 2. Fine bore: – for long-term use. – should be changed every 30 days. In general, tube sizes of 6 Fr are used for standard feeds, and 7-10 Fr for higher density and fibre feeds. Tubes come in a range of lengths, usually 55cm, 75cm or 85cm. Wash and dry hands thoroughly. Place all the equipment needed on a clean tray. • Find the most appropriate position for the child, depending on age and/or ability to co operate. Older children may be able to sit upright with head support. Younger children may sit on a parent’s lap. Infants may be wrapped in a sheet or blanket. • Check the tube is intact then stretch it to remove any shape retained from being packaged. • Measure from the tip of the nose to the bottom of the ear lobe, then from the ear lobe to xiphisternum. The length of tube can be marked with indelible pen or a note taken of the measurement marks on the tube (for neonates: measure from the nose to ear and then to the halfway point between xiphisternum and umbilicus). • Lubricate the end of the tube using a water-based lubricant. • Gently pass the tube into the child’s nostril, advancing·1along the floor of the nasopharynx to the oropharynx. Ask the child to swallow a little water, or offer a younger child their soother, to assist passage of the tube down the oesophagus. Never advance the tube against resistance. • If the child shows signs of breathlessness or severe coughing, • remove the tube immediately. Lightly secure the tube with tape until the position has been checked
Text C
Text D:
Administering feeds/fluid via a feeding tube Feeds are ordered through a referral to the dietitian. When feeding directly into the small bowel, feeds must be delivered continuously via a feeding pump. The small bowel cannot hold large volumes of feed. Feed bottles must be changed every six hours, or every four hours for expressed breast milk. Under no circumstances should the feed be decanted from the container in which it is sent up from the special feeds unit. All feeds should be monitored and recorded hourly using a fluid balance chart. If oral feeding is appropriate, this must also be recorded. The child should be measured and weighed before feeding commences and then twice weekly. The use of this feeding method should be re-assessed, evaluated and recorded daily.
We hope this information has been valuable to you. If so, please consider a monetary donation to Lifestyle Training Centre via UPI. Your support is greatly appreciated.
Would you like to undergo training for OET, PTE, IELTS, Duolingo, Phonetics, or Spoken English with us? Kindly contact us now!
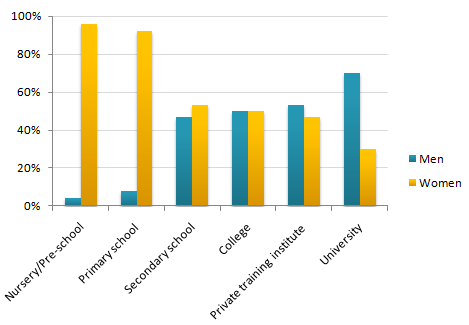
Question: 29 The chart below shows the percentage of male and female teachers in six different types of educational setting in the UK in 2010. Summarise the information by selecting and reporting the main features, and make comparisons where relevant.
Model answer by Lifestyle Training Centre
The given bar chart illustrates gender wise percentage distribution of male and female teachers among six various kinds of academic settings in the United Kingdom in the year 2010.
Overall, it is evident that the proportion of men increases noticeably as the academic level rises. Conversely, the percentage of women who are employed in lower academic levels are substantially higher, presenting a stark contrast with men.
In Nursery/Pre-school, around 3% of teachers are male and the remaining 97% females. Likewise, primary school consists of around 7% male tutors and 93% female. In secondary school, around 47 % of teachers are male and the remaining 53% female. Interestingly, at college level, the gender wise distribution of teachers are equal: 50% each.
Private training institute consists of around 53% male and 47% female faculties. At university level, around 70% of the faculties are male, while less than half of the strength, 35%, are female.
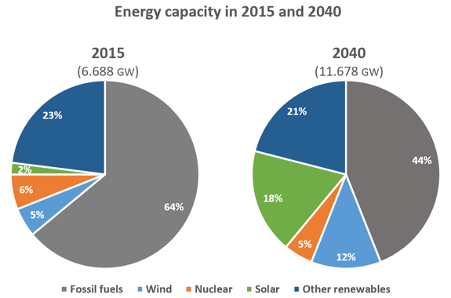
The pie charts below compare the proportion of energy capacity in gigawatts (GW) in 2015 with the predictions for 2040.Summarise the information by selecting and reporting the main features, and make comparisons where relevant.
Model answer by Lifestyle Training Centre
The provided two pie charts compare the percentage of energy produced in 2015 with the projected figures for 2040, across various sources including fossil fuels, wind, nuclear, solar, and other renewables. The energy capacity is delineated in gigawatts (GW).
Overall, it is evident that fossil fuels and other renewables remain the major energy contributors throughout the given period. Moreover, solar and wind energy are predicted to increase substantially in the future.
The aggregate capacity in 2015 was 6.688 GW, which is expected to almost double to 11.678 GW by 2040. Fossil fuels covered 64% of the energy capacity, which will undergo a considerable downturn to a mere 44% by the year 2040. Other renewables and nuclear, however, are expected to only experience a marginal decline in energy production: the former from 23% in 2015 to 21% by 2040, and the latter from 6% in 2015 to 5% in 2040.
Conversely, both solar and wind energy are estimated to soar remarkably – solar from 2% in 2015 to a staggering 18% by 2040, and wind energy from 5% in 2015 to 12% by 2040.
We hope this information has been valuable to you. If so, please consider a monetary donation to Lifestyle Training Centre via UPI. Your support is greatly appreciated.
Would you like to undergo training for OET, PTE, IELTS, Duolingo, Phonetics, or Spoken English with us? Kindly contact us now!
Text A. Autism Spectrum Disorder: Autism Spectrum Disorder {ASD) develops in early childhood. Recent population analysis indicates that the number of cases of ASD is increasing in many countries, particularly in technologically developed countries. The U.S. Center for Disease Control research claims that, in some states, one of every 68 children {one of 42 boys) has a diagnosis of the ASD, a 30% increase from 2012 {IACC Strategic Plan for Autism Spectrum Disorder Research, 2013.
Multiple dysfunctional reflex patterns are characteristic in two separate groups of children diagnosed with autism: 1) those whose patterns were immature or pathological and severely dysfunctional from birth, and 2) those that developed normally but regressed into autism at age 2 or 3 unexpectedly. Reflexes of these children may have been delayed and immature, but not noted by specialists or parents. Their nerve system, possibly, was not resilient enough to cope with the stress that they experienced. Alternatively, their reflexes might not have matured and have caused the asynchronicity in their brain function development on both cortical and extrapyramidal levels resulting in neurodevelopmental disorders beginning around 2 years of age. An initially mild unrecognized problem can lead to more complicated deficits with age.
Text B: Individuals diagnosed with ASD show a chronic lack of sensory motor integration and delay of skills concerning the early motor milestones. They show a wide range of immature reflex patterns such as Hands Pulling, Hands Supporting, Hands Grasp, Crawling, Asymmetrical Tonic Neck Reflex, Symmetrical Tonic Neck Reflex, Babkin Palmomental, Ocular-Vestibular, and other patterns. The MNRI program utilizes non-invasive intervention to support the development of the neuro-sensory-motor aspects of those reflex patterns through specific techniques and procedures that allow restoration of links between reflex circuit components and the protection function of a reflex to normalize their over-freezing and fight or flight reactions seen, for example, in tactile defensiveness or deprivation. Thus, the MNRI program works particularly with the autonomic nervous system – its sympathetic and parasympathetic processes.
Text C: Disharmony in muscular system development and lack of regulation for muscle tone beginning in children with ASD in their infancy results in impulsive reactions that often turns into permanent physical characteristics and behaviors as they grow older. For example, impulsivity may lead to poor ability for goal setting, poor focus and following instructions, deficient inner control, hyperactivity, disorganized and chaotic behavior, and irritability and impatience. Lack of muscle tone regulation may later result in challenges in motor programming and control, planning, and thus lead to poor motor-cognitive- behavior coordination. This poor regulation is caused by a lack of balance in the excitation and inhibition processes in the reflex circuits, including improper connectivity between alpha and gamma motor neurons. Clinical observations show that the disharmony and lack of proper regulation in muscle tone in children with ASD are seen mainly in: Hypertonic muscles in the posterior dorsal plane of the body {along the spinal column – sacrospinalis, thoracic longus, trapezius) and with the opposite hypotonic abdominal muscles and diaphragm negatively affects development of postural control. The child with ASD, in an attempt to release tension caused by this disproportion of muscle tone in the back and front of their body, may often display reactivity in behavior and impulsive movements triggering balance/equilibrium mechanisms {balancing reflex pattern), resulting in a state of being overstimulated.
Text D: Problems in visual and auditory perception systems:
The eyes of children diagnosed with ASD show a restless state or lack of mobility and dilated pupils. They usually have a limited, narrow visual span, poor visual attention and focus, and hyperactive peripheral vision. Their eye movements appear to freeze or jump rapidly in saccades. Many children with ASD demonstrate an addictive tendency for computers and cell phones with compulsive repetition of the same image, object, or program, often watching it at a very close range. The child with ASD becomes over-focused, which over-stimulates their vestibular system and static balance. The Pupillary Reflex in these children may become hypersensitive, overstimulating the sympathetic system, with either over-reactive or hypoactive motor activity. The visual system of children diagnosed with ASD copes poorly with this visual chaos which leads to a visual processing disorder. A Bonding response in infants is seen from their first months after birth. Bonding as a behavior trait matures during their first years of life. Almost every child with ASD assessed presented signs of inadequate bonding – lack of attachment, tactile and interactivity defensiveness, a tendency for self-isolation, a poor imitation, and poor learning of verbal communication. When bonding is immature, there are problems with visual contact, focusing on the face/eyes of their mother and other adults and poor emotional communication, inability to adequately smile, and poor labeling of the objects in their environment.
PART A -QUESTIONS AND ANSWER SHEET. Questions 1-7. For each question, 1-7, decide which text {A, B, C or D) the information comes from. You may use any letter more than once. In which text can you find information about;
1. Represents the resistance to passive movement of a joint. Answer
2. Associated with pupillary function. Answer
3. Utilization of information and clinical experience from neurodevelopment in different ways. Answer
4. Development of autism. Answer
5. Possibility of development of strange characteristics as one grows. Answer
6. Not existing or occurring at the same time with respect to movements or reactions. Answer
7. Primitive reflex that normally emerges during the first year of an infant’s life. Answer
Questions 8-14. Answer each of the questions, 8-14, with a word or short phrase from one of the texts. Each answer may include words, numbers or both. Your answers should be correctly spelt.
8. What MNRI will operate with? Answer
9. How eye movements may appear? Answer
10. What is the term which defines activation of the vestibular system which causes eye movement? Answer
11. What is related to tendency to act on a whim, displaying behaviour characterized by little or no forethought, reflection? Answer
12. What is the term used to define healthy stress? Answer
13. What is known to be activated as a result of turning the head to one side? Answer
14. What is the impact visual chaos of the children with ASD? Answer
Questions 15-20. Complete each of the sentences, 15-20, with a word or short phrase from one of the texts. Each answer may include words, numbers or both. Your answers should be correctly spelt.
15. The term is used to describe a rapid movement of the eye between fixation points.
16. Generally, in newly born babies will be at very early stages.
17. What synchronizes hands, neck, and jaw is
18. In many of the cases, reflex in affected children may turn out to be more .
19. Almost all of the children with ASD show various signs of .
20. The complexities in can be the result of the regulation changes in muscle tone.
READING SUB-TEST : PART B. Questions 1-6
1. What this notice talks about?
A. AIDS-related deaths dropped by more than 50%
B. AIDS-related deaths increased more significantly
C. Efforts that can lead to curbing AIDS in various countries.
UNAIDS Programme Coordinating Board
The 31st UNAIDS Programme Coordinating Board {PCB) meeting took place in Geneva from 11-13 June 2018. There were more than 700 000 less new HIV infections estimated globally in 2016 than in 2001. The road from 2.5 million new HIV infections in 2011 to zero new HIV infections is a long one and significant efforts are required to accelerate HIV prevention programmes. Sustained investments for access to antiretroviral therapy by donors and national governments have led to record numbers of lives being saved in the past six years.
In 2011 more than half a million fewer people died from AIDS-related illnesses than six years earlier. It’s a dramatic turning point. Numbers can quantify, but alone cannot express the impact of each averted death on the whole community, including its children. The number of people dying from AIDS-related causes began to decline in the mid-2000s because of scaled up antiretroviral therapy and the steady decline in HIV incidence since the peak of the epidemic in 1997. In 2011, this decline continued, with evidence showing that the drop in the number of people dying from AIDS-related causes is accelerating in several countries.
2. The given notice explains the procedure of;
A. Use of radix Sophorae samples.
B. Ultrasonic treatment – obtaining radix.
C. Preparing radix Sophorae tonkinensis samples.
Radix Sophorae tonkinensis: Radix Sophorae tonkinensis was crushed and screened, then taking screened powder (approximately 0.5 g) gain a respective weight, denoted M. Trichloromethane-methanol- ammonia (40:10:1) was used to dispose of the radix Sophorae tonkinensis samples for 30 min, and all samples were subsequently obtained from organic solvent extraction with 30 min ultrasonic treatment. All disposed of samples were filtered, then 10 ml of filtrate was measured to recover solvents to dry under decompression at 38°C to obtain the residue, the residue was diluted by methanol, then transferred to a 10 ml volumetric flask. After mixing and filtering with 0.45 µm filter membrane, Radix Sophorae samples were obtained. The blank groups were treated as the samples but without radix Sophorae tonkinensis.
3. What is correct about Torcetrapib?
A. It is known to enhance health.
B. Trials performed produced negative results.
C. The drug did not get approved completely as the project was dropped in the middle.
Short note on Torcetrapib: Torcetrapib, which has been in development since the early 1990s, was supposed to raise so-called good cholesterol, and cardiologists had hoped it would reduce the buildup of plaques in blood vessels that can cause heart attacks. This drug actually caused an increase in deaths and heart problems. Eighty-two people had died so far in a clinical trial, versus 51 people in the same trial who had not taken it. The GABR company gave up the project incurring a claimed loss of $1 billion investment and not much hue and cry was raised on the deaths of the study subjects as this was the doing of a billionaire giant manufacturer.In case of trials or experiments, if a single death is noticed with the use of UD, a big hue and cry would be raised.
4. The table shows
A. Comparison of Type A, B, C and G and H drugs and their resistance quality.
B. Type A is known to produce more adverse reactions than all the others present in the table.
C. A total of 200 cases have been reported with respect to adverse reaction.
Drug Adverse Reactions
Type of ADR
Number ADRS
Percentage {%)
Type-A
96
103.7
Type-B
69
56.79
Type-C
23
28.39
Type G
8
7.4
Type H
4
3.7
Total
200
200
5. The notice clearly explains
A. Clinical trials using Vitamin B12.
B. Advantages of B12.
C. Study performed with focus on B12 usage.
Vitamin B12: Vitamin B12 is produced by the liver and is involved in several biochemical metabolic reactions. It promotes the repair of damaged skin mucous membranes and vascular endothelial cells, reduces spasm and occlusion of blood vessels, improves local blood flow and prevents the deterioration of wound infection. In addition, it reduces the excitability of pain fibers C and AG, leading to an analgesic effect. Vitamin B12 injections to the skin in the radiation field benefit the wound by reducing irritation and pain, preventing rupture and enhancing new epithelial resistance to radiation, thereby promoting healing of the skin.
Chen et al used a vitamin B12 solution to treat radiation-induced moist dermatitis. The cure rate at 10 days was 100%, which was significantly different from the control group.
6. What is correct about the given table?
A. The age wise male patients population ranges from 4.
B. 18.18 patients were in the age group of 50-70 years.
C. 32.72 patients were in the age group of 50-60 years.
Age wise distribution of male patients showing percentage of distribution.
Age in years
Male patients
Age in years
Femalepatients
20-30
4 (7.27)
20-30
0 (0)
30-40
54 (98.18)
30-40
32 (71.11)
40-50
24 (43.63)
40-50
38
50-60
18
50-60
10
60-70
10
60-70
6 (13.32)
Total
110 (110)
70-80
4 (8.88)
Total
90 (9
READING SUB-TEST : PART C In this part of the test, there are two texts about different aspects of healthcare.For questions 7-22, choose the answer {A, B, C or D) which you think fits best according to the text. Write your answers on the separate Answer Sheet
Text 1: Ebola Virus and Marburg Virus
The Ebola virus and Marburg virus are related viruses that cause hemorrhagic fevers; illnesses marked by severe bleeding {hemorrhage), organ failure and, in many cases, death. Both the Ebola virus and Marburg virus are native to Africa, where sporadic outbreaks have occurred for decades. The Ebola virus and Marburg virus both live in animal hosts, and humans can contract the viruses from infected animals. After the initial transmission, the viruses can spread from person to person through contact with bodily fluids or contaminated needles.
No drug has been approved to treat the Ebola virus or Marburg virus. People diagnosed with the Ebola or Marburg virus receive supportive care and treatment for complications. Scientists are coming closer to developing vaccines for these deadly diseases. In both the Ebola virus and Marburg virus, signs and symptoms typically begin abruptly within the first five to 10 days of infection. Early signs and symptoms include fever, severe headaches, joint and muscle aches, chills, sore throat and weakness. Over time, symptoms become increasingly severe and may include nausea and vomiting, diarrhea {may be bloody), red eyes, raised rash, chest pain and coughing, stomach pain, severe weight loss, bleeding from the nose, mouth, rectum, eyes and ears.
The Ebola virus has been found in African monkeys, chimps and other nonhuman primates. A milder strain of Ebola has been discovered in monkeys and pigs in the Philippines. The Marburg virus has been found in monkeys, chimps and fruit bats in Africa. The virus can be transmitted to humans by exposure to an infected animal’s bodily fluids, including blood. Butchering or eating infected animals can spread the viruses; scientists who have operated on infected animals as part of their research have also contracted the virus. Infected people typically don’t become contagious until they develop symptoms. Family members are often infected as they care for sick relatives or prepare the dead for burial.
Medical personnel can be infected if they don’t use protective gear such as surgical masks and latex gloves. Medical centers in Africa are often so poor that they must reuse needles and syringes and some of the worst Ebola epidemics have occurred because contaminated injection equipment wasn’t sterilized between uses. There’s no evidence that the Ebola virus or Marburg virus can be spread via insect bites.
Ebola and Marburg hemorrhagic fevers are difficult to diagnose because many of the early signs and symptoms resemble those of other infectious diseases, such as typhoid and malaria. But if doctors suspect that you have been exposed to the Ebola virus or Marburg virus, they use laboratory tests that can identify the viruses within a few days.
Most people with Ebola or Marburg hemorrhagic fever have high concentrations of the virus in their blood. Blood tests known as enzyme-linked immunosorbent assay (ElISA) and reverse transcriptase polymerase chain reaction (PCR) can detect specific genes or the virus or antibodies to them. No antiviral medications have proved effective in treating the Ebola virus or Marburg virus infections. As a result, treatment consists of supportive hospital care; this includes providing fluids, maintaining adequate blood pressure, replacing blood loss and treating any other infections that develop.
As with other infectious diseases, one of the most important preventive measures for the Ebola virus and Marburg virus is frequent hand-washing. Use soap and water, or use alcohol-based hand rubs containing at least 60 percent alcohol when soap and water aren’t available. In developing countries, wild animals, including nonhuman primates, are sold in local markets; avoid buying or eating any of these animals. In particular, caregivers should avoid contact with the person’s bodily fluids and tissues, including blood, semen, vaginal secretions and saliva. People with Ebola or Marburg are most contagious during the later stages of the disease. If you’re a healthcare worker, wear protective clothing – such as gloves, masks, gowns and eye shields – keep infected people isolated from others. Carefully disinfect and dispose of needles and other instruments; injection needles and syringes should not be reused. Scientists are working on a variety of vaccines that would protect people from Ebola or Marburg viruses. Some of the results have been promising, but further testing is needed.
Text 1: Questions 7-14
7. The Ebola and Marburg Viruses are native to;
A. America
B. Japan
C. Africa
D. China
8. What is right about Ebola and Marburg viruses?
A. Spread from person to person only.
B. Spread from animals to humans.
C. Spread from animals to animals.
D. Spread person to person after initial transmission from the infected animals.
9. Symptoms are typically seen within;
A. Five days
B. Ten days
C. Five to seven days
D. Five to ten days
10. In the Philippines, Ebola was discovered in;
A. Chimpanzees
B. Human primates
C. Non-human primates
D. Monkeys
11. Most known Ebola diseases occur due to;
A. Contamination
B. Bodily fluids
C. Contaminated needles and syringes
D. None
12. People with hemorrhagic fever show;
A. High number of viruses in their blood
B. Low concentrations of virus
C. High concentrations of antibodies
D. Low concentrations of antibodies
13. Pick one of the best preventive measures stated in the passage here;
A. Hand cleaning with medicinal soap.
B. Use of alcohol-based hand rubs, containing at least 60% alcohol, in absence of water & soap.
C. Only use of soap.
D. Avoiding direct contact with patients is a necessity.
14. As a healthcare worker, you should;
A. Keep infected people totally isolated from others.
B. Not reuse needles and syringes for the second time.
C. Wear clothing such as gowns and eye shields.
D. none of the above
Text 2: A Chronic Disease – Atopic Dermatitis
Atopic dermatitis is a common chronic skin disease. It is also called atopic eczema. Atopic is a term used to describe allergic conditions such as asthma and hay fever. Both dermatitis and eczema mean inflammation of the skin. People with atopic dermatitis tend to have dry, itchy and easily irritated skin. They may have times when their skin is clear and other times when they have rash. In infants and small children, the rash is often present on the skin around the knees and elbows and the cheeks. In teenagers and adults, the rash is often present in the creases of the wrists, elbows, knees or ankles, and on the face or neck.
Atopic dermatitis usually begins and ends during childhood, but some people continue to have the disease into adulthood. If you have ever had atopic dermatitis, you may have trouble with one or more of these: dry, sensitive skin, hand dermatitis and skin infections. The exact cause of atopic dermatitis is unknown.
Research suggests that atopic dermatitis and other atopic diseases are genetically determined; this means that you are more likely to have atopic dermatitis, food allergies, asthma and/or hay fever if your parents or other family members have ever had atopic dermatitis. These diseases may develop one after another over a period of years. This is called the “atopic march”.
Knowing that a child with a slight wheeze has had a history of atopic dermatitis, for example makes it easier to diagnose the subtle onset of asthma. There are many things that make the itching and rash of atopic dermatitis worse. When you learn more about atopic dermatitis and how to avoid things that make it worse, you may be able to lead a healthier life.
If you have a reaction to something you touch, breathe or eat, you might have an allergy. Allergies can trigger or worsen your atopic dermatitis symptoms. Common causes of allergy are: dust mites, furry and feathered animals, cockroaches, pollen, mold, foods, chemicals. Your healthcare provider may recommend allergy testing and food challenges to see if allergies worsen itching or rashes. Allergy testing may include skin testing, blood tests or patch tests. Many measures can be taken to avoid things to which you are allergic. Although many of the measures can be done for the entire home, the bedroom is the most important room to make skin friendly. Talking with healthcare provider about what measures you can take to avoid your allergens can be very beneficial.
Food allergies may be the cause of itching or rashes that occur immediately after eating, especially in children. Some common food allergens include milk, eggs, peanuts, wheat, nuts, soy and seafood. Most people are allergic to only one, two or at the most three foods. Be aware that diet restrictions can lead to poor nutrition and growth delay in babies and children. Talk with your healthcare provider about maintaining a well-balanced diet.
Emotions and stress do not cause atopic dermatitis, but they may bring on itching and scratching. Anger, frustration and embarrassment can cause flushing and itching. Day to day stresses as well as major stressful events can lead to or worsen the itch-scratch cycle.The medications used in atopic dermatitis include topical steroids, topical immunomodulators, tar products, anti-infectives and antihistamines. Steroid medicines that are applied to the skin are called topical steroids. Topical steroids are drugs that fight inflammation; they are very helpful when a rash is not well controlled. Topical steroids are available in many forms such as ointments, creams, lotions and gels. It is important to know that topical steroids are made in low to super potent strengths. Steroid pills or liquids, like prednisone, should be avoided because of side effects and because the rash often comes back after they are stopped.
Text 2: Questions 15-22
15. People with atopic dermatitis suffer from;
A. Hay fever
B. Asthma
C. Dry, itchy and irritated skin
D. Rashes
16. In small children, a rash is seen;
A. Around elbows
B. On the face
C. On the neck
D. Around the knees
17. People with atopic dermatitis have;
A. Dry skin
B. Skin infections
C. Hand dermatitis
D. All of the above
18. The term atopic refers to;
A. Allergic diseases
B. Asthma and hay fever.
C. Allergic conditions like hay fever.
D. Allergic conditions like asthma.
19. can worsen dermatitis symptoms;
A. Allergies
B. Pollen
C. Dust
D. Mold
20. According to the information given in the passage, avoiding allergens is;
A. Easy
B. Difficult
C. Sometimes easy and sometimes difficult
D. Can say
21. Allergic conditions like asthma in patients who have had a history of atopic dermatitis can be easily diagnosed by health professionals, this statement is;
A. Out of the paragraphs given
B. False
C. True
D. Can be true or can be false
22. Topical steroids are available in these forms:
We hope this information has been valuable to you. If so, please consider a monetary donation to Lifestyle Training Centre via UPI. Your support is greatly appreciated.
Would you like to undergo training for OET, PTE, IELTS, Duolingo, Phonetics, or Spoken English with us? Kindly contact us now!